

Background: The back of the head is exposed to numerous deforming forces both in utero as well as after birth. Given that laying on the back of the head is necessary to some degree in many non-vertical positions, the early influences of positioning in utero and early in the first year of life on soft and thin cranial bones can make for an occipital plagiocephaly type skull deformity.
While helmet therapy can really help the plagiocephalic patient early on, once the bone thickens the skull shape is locked in for all time. Its degree of severity will determine whether it is a largely isolated asymmetry to the back of the head or has obvious manifestations that extend to the forehead, face and ears.
Heretofore, correction of occipital plagicephay is adults has been viewed as untreatable or unimportant enough that surgery was not ‘warranted’. And when viewed as changing the shape of the bone through osteotomies and repositioning, that would certainly be true. But to those so affected, a treatment that would be effective without all the risks of actual skull bone surgery would be welcome.
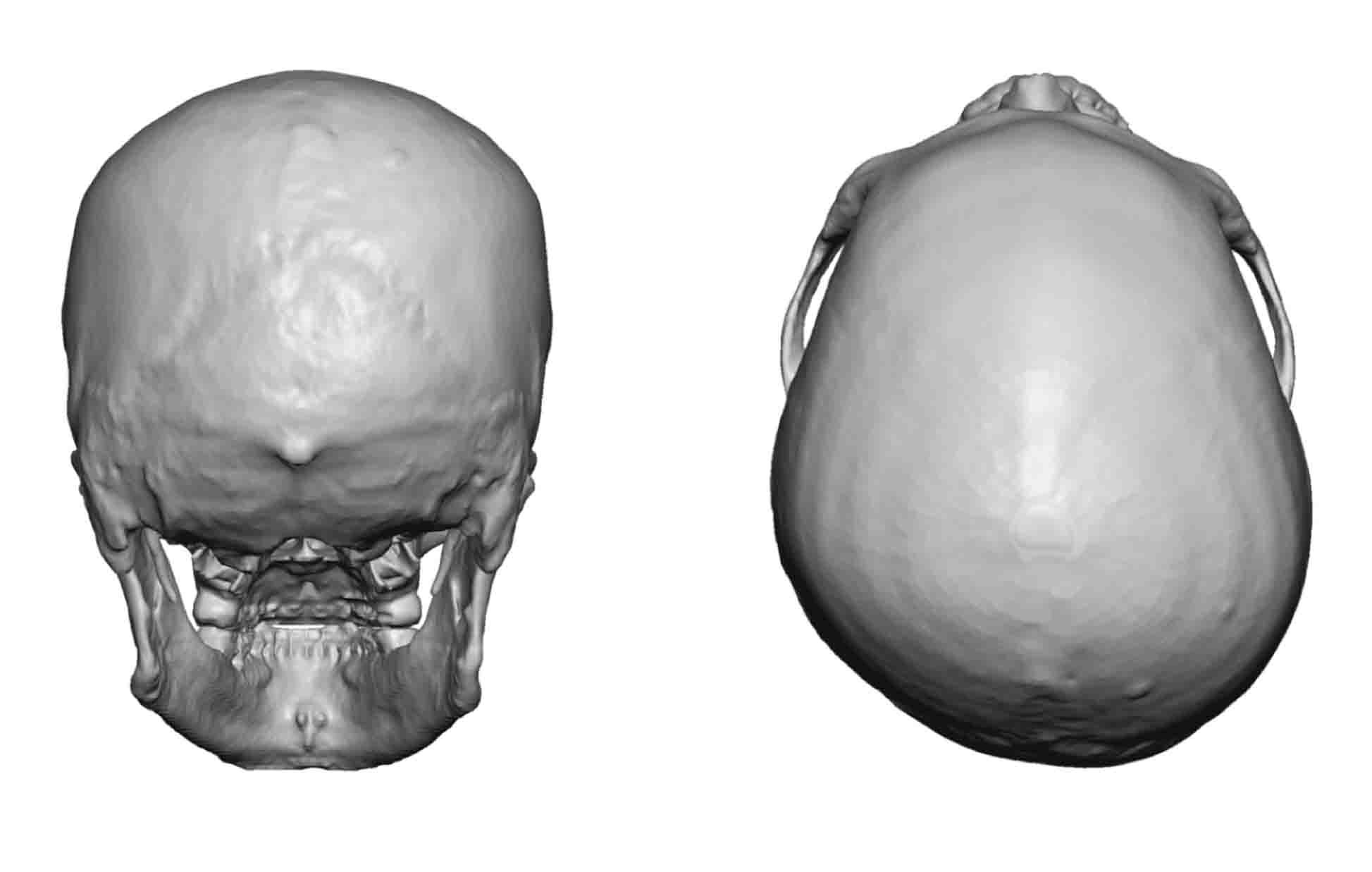 Case Study: This adult male had a left-sided occipital plagiocephaly that had bothered him for a long time. Wearing short hair clearing showed the much flatter side of the back of the head. It was as if a part of the back of his head was missing. A 3D CT scan showed the extent of the skull deformity with some mild compensatory bulging in the right posterior parietal-temporal area.
Case Study: This adult male had a left-sided occipital plagiocephaly that had bothered him for a long time. Wearing short hair clearing showed the much flatter side of the back of the head. It was as if a part of the back of his head was missing. A 3D CT scan showed the extent of the skull deformity with some mild compensatory bulging in the right posterior parietal-temporal area.
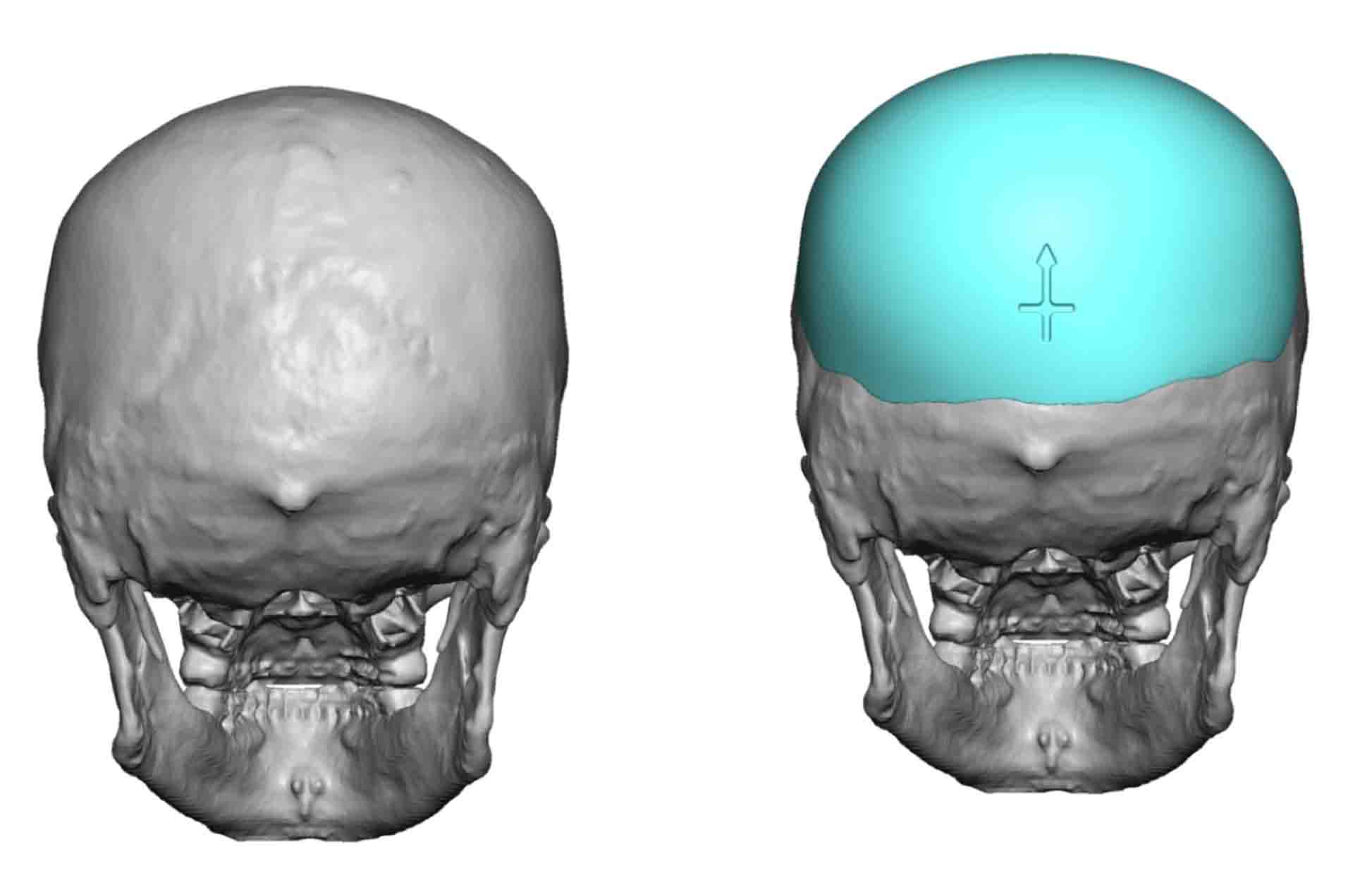 From the 3D CT scan, a custom occipital skull implant was designed. Its design showed that creating a bony symmetry on the back of the head involved than just building out the flattened left side of the face.
From the 3D CT scan, a custom occipital skull implant was designed. Its design showed that creating a bony symmetry on the back of the head involved than just building out the flattened left side of the face.
 Under general anesthesia, an 8 cm horizontal scalp incision was made over the nuchal ridge on the back of the head in the prone position. A wide subperiosteal pocket was made beyond the implant’s bone coverage areas. The implant was inserted using a rolled technique that was unrolled once inside the pocket and positioned.
Under general anesthesia, an 8 cm horizontal scalp incision was made over the nuchal ridge on the back of the head in the prone position. A wide subperiosteal pocket was made beyond the implant’s bone coverage areas. The implant was inserted using a rolled technique that was unrolled once inside the pocket and positioned.

 It is difficult if not impossible to match the accuracy of a computer-designed skull implant in occipital plagiocephaly. Besides the larger scalp incision needed for the more conventional use of bone cements, visual shaping of an asymmetric skull shape is never as good as what a preformed computer-based implant can do.
It is difficult if not impossible to match the accuracy of a computer-designed skull implant in occipital plagiocephaly. Besides the larger scalp incision needed for the more conventional use of bone cements, visual shaping of an asymmetric skull shape is never as good as what a preformed computer-based implant can do.
Case Highlights:
1) Contour deformities of the back of the head are common are often asymmetric in shape.
2) While occipital plagiocephalies are often viewed as flatness on one side of the head, a more complete correction often requires crossing the midline.
3) A discrete and limited scalp incision is one of the important goals of occipital plagiocephaly correction with a custom skull implant.
Dr. Barry Eppley
Indianapolis, Indiana