

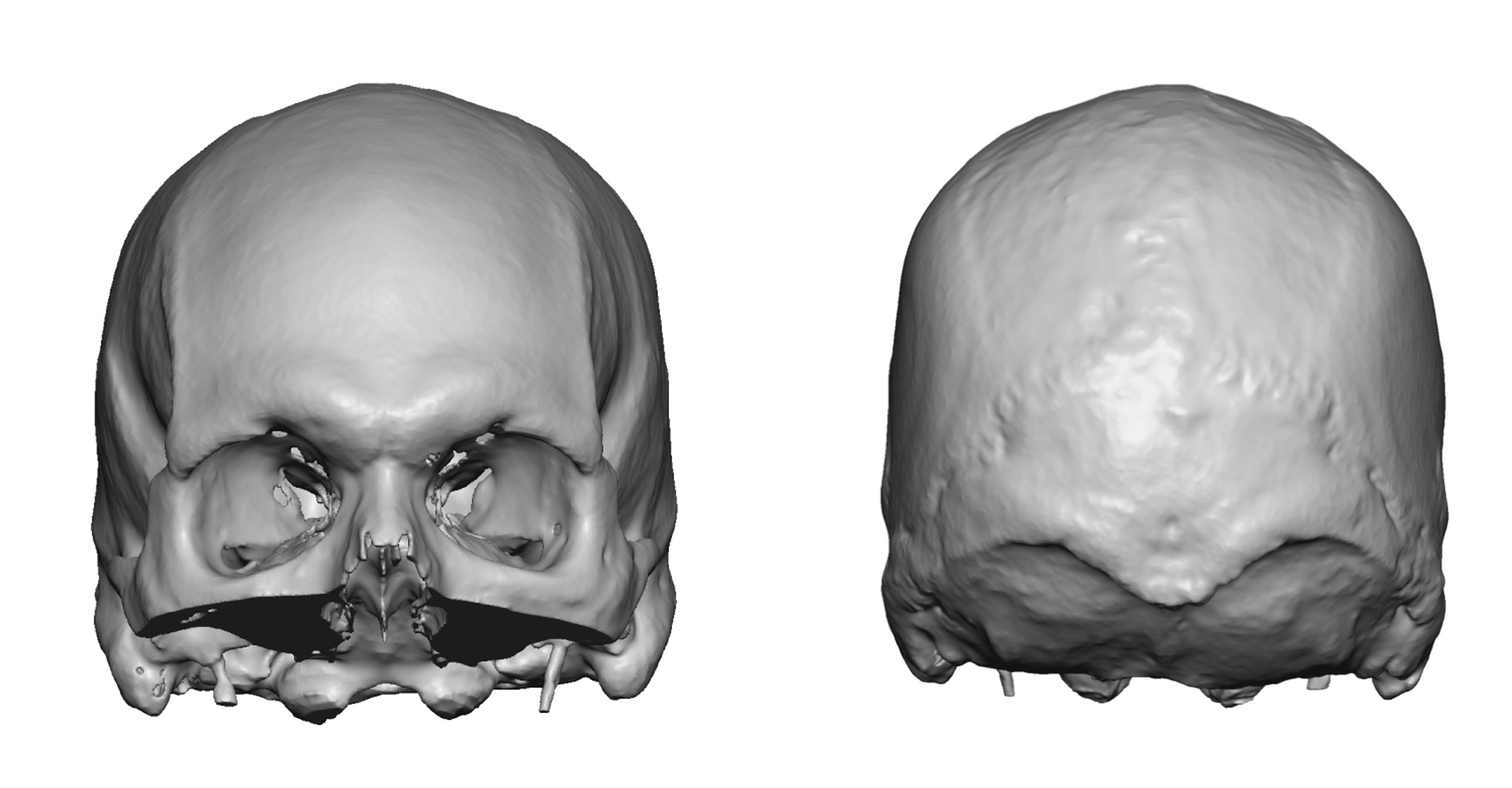
Background: A sagittal ridge skull deformity is most commonly perceived as its fullest expression with sagittal craniosynotosis in an infant. But there are greater numbers of patients affected by lesser or more ‘aesthetic’ sagittal deformities where the height of the sagittal crest and the degree of parasagittal depression along the sides is much less severe. These may be known as microforms of sagittal craniosynostosis. But are probably better viewed as merely the range of shapes that can occur when a complex structure like a cranial suture must develop and eventually fuse.
The sagittal crest deformity is an adult manifestations of a raised bony ridge down the center of the head. It comes in degrees of manifestations with a linear relationship between the height of the ridge and the degree of parasagittal inclination along its sides. This is almost exclusively seen in the adult male patient who has thin hair or shaves his head where the shape or profile of the top of the head becomes a more prominent aesthetic feature.
The aesthetic treatment of a sagittal crest depends on its height. More moderate sagittal crests can be reduced by burring only. But whether become higher and the parasagittal shape becomes more inclined, midline burring alone is not going to create a more pleasing skull profile from the frontal view. The parasagittal area must be built up as well, usually done with a custom skull implant to complement the bony ridge reduction. Together, midline down and the sides up, can a more pleasing convex shape to the top of the head be achieved.
 Case Study: This young male initially presented with a history of having had a prior undiagnosed sagittal crest skull deformity that was treated by ‘exploratory surgery’ and a biopsy/soft tissue removal. This did not produce an aesthetic change. I initially performed a bony sagittal ridge reduction which we thought would be adequate for eliminating the visible midline peak. While better he desired further improvement for a rounder skull shape. A secondary procedure was then performed placing a custom skull implant with a horseshoe-shaped design to augment the parasagittal areas as well as the upper occiput. While better there remained some differences in height between the two parasagittal areas.
Case Study: This young male initially presented with a history of having had a prior undiagnosed sagittal crest skull deformity that was treated by ‘exploratory surgery’ and a biopsy/soft tissue removal. This did not produce an aesthetic change. I initially performed a bony sagittal ridge reduction which we thought would be adequate for eliminating the visible midline peak. While better he desired further improvement for a rounder skull shape. A secondary procedure was then performed placing a custom skull implant with a horseshoe-shaped design to augment the parasagittal areas as well as the upper occiput. While better there remained some differences in height between the two parasagittal areas.
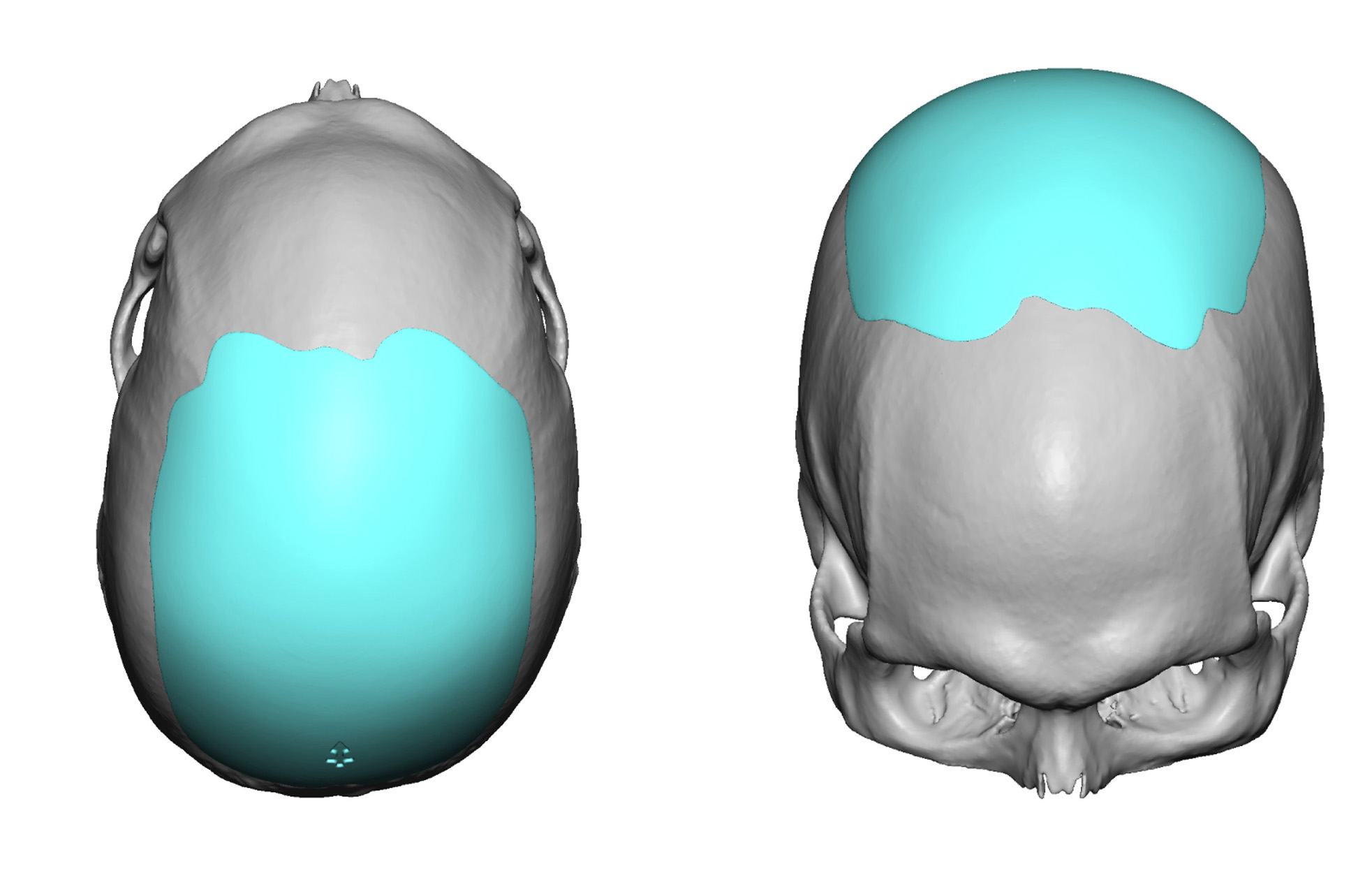
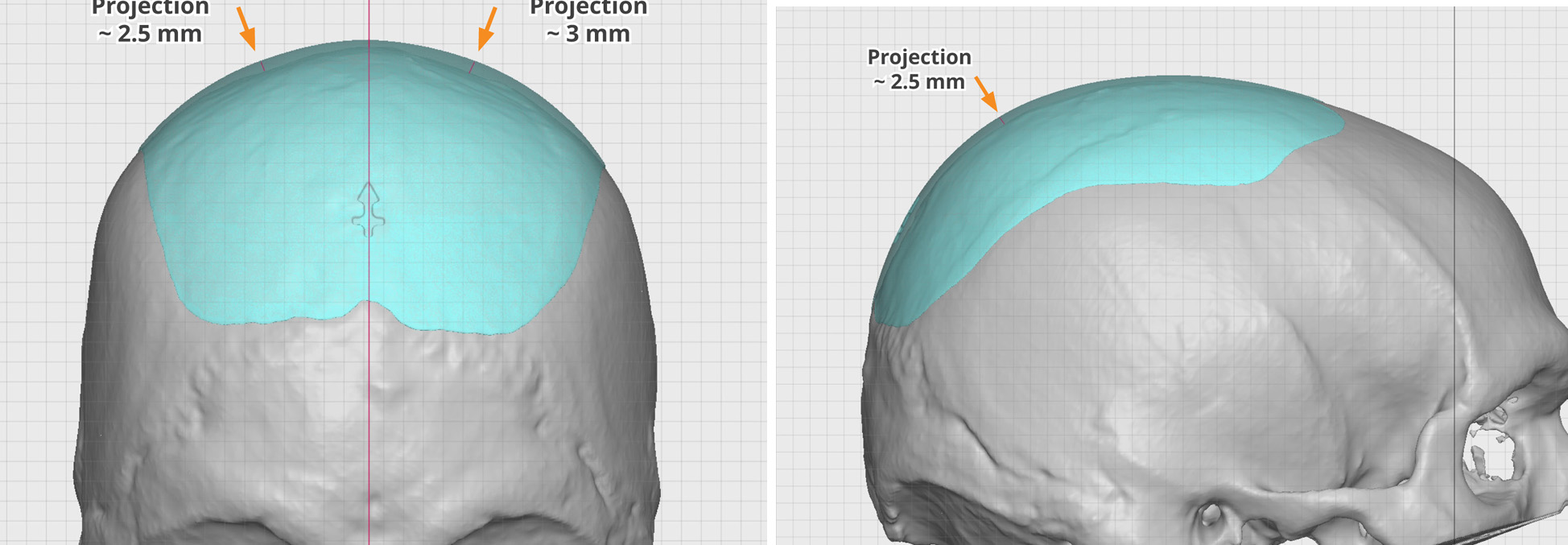 It was then decided to do a second custom skull implant to cover the entire upper skull surface by making the part of the implant that crossed the middle to be very thin. Thus was felt to be the best approach to getting a uniform skull shape. This was a very thin implant even in the parasagittal region.
It was then decided to do a second custom skull implant to cover the entire upper skull surface by making the part of the implant that crossed the middle to be very thin. Thus was felt to be the best approach to getting a uniform skull shape. This was a very thin implant even in the parasagittal region.
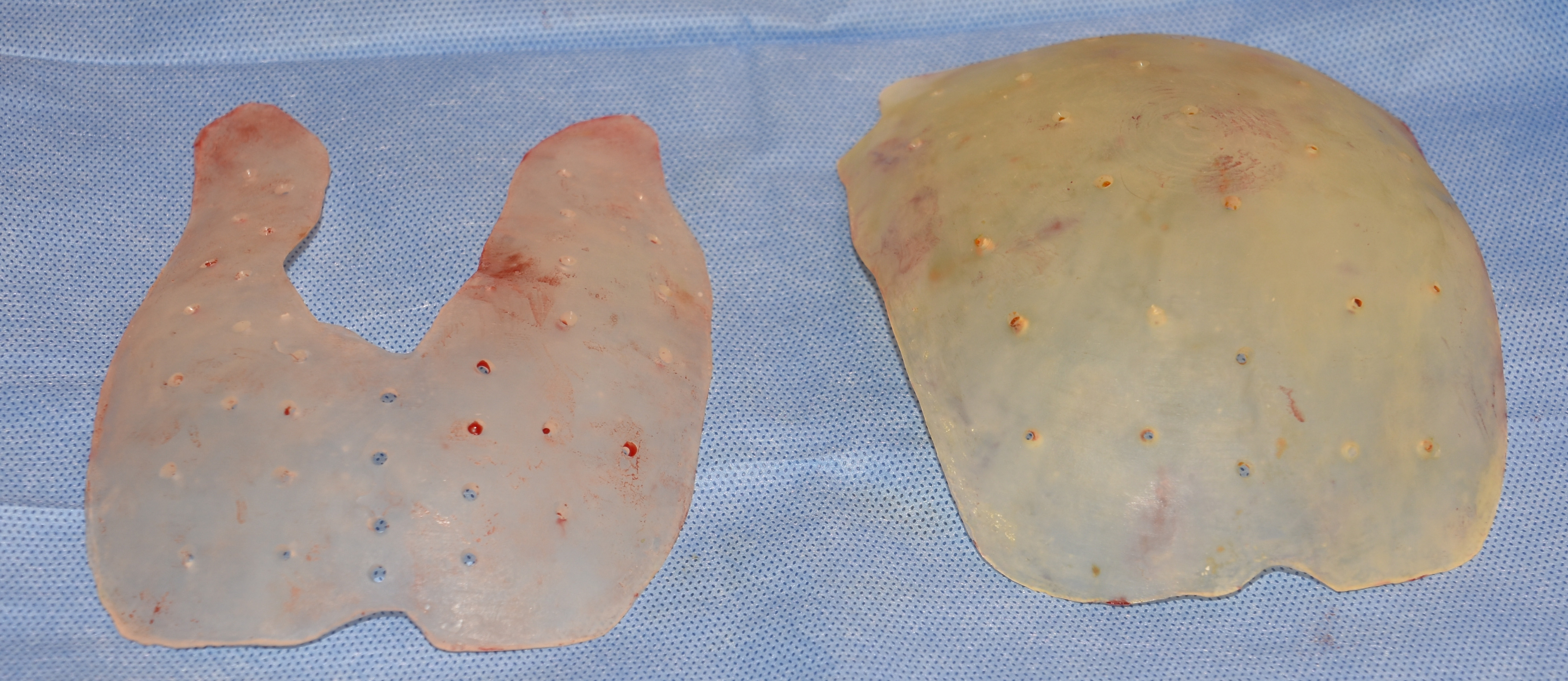 Under general anesthesia the old custom skull implant was remember and replaced through his existing midline 7cm sagittal incision from his original exploratory surgery. A comparison of the old and new skull implants showed the thin but complete connection between the two halfs of the old implant.
Under general anesthesia the old custom skull implant was remember and replaced through his existing midline 7cm sagittal incision from his original exploratory surgery. A comparison of the old and new skull implants showed the thin but complete connection between the two halfs of the old implant.
In more significant sagittal crest deformities the combination of a bony sagittal ridge reduction and parasagittal augmentation is usually the most effective approach to a more convex skull shape. But this involves a harmonious surface contour between three variables which in this case did not work to the patient’s aesthetic satisfaction. Changing to a complete skull implant design eventually created the best aesthetic result.
Highlights:
1) A smooth convex skull shape may not always result from the bony reduction of a prominent sagittal ridge.
2) The combined approach of a sagittal ridge reduction and a custom horse-shaped skull implant is effective the the sagittal ridge is more prominent.
3) When the perfect convex shape is not achieved by the combination of sagittal bone reduction and building up along the sides (parasagittal augmentation) then a custom skull implant that covers the complete top of the head may be needed.
Dr. Barry Eppley
Indianapolis, Indiana