

Background: The most successful approach to skull augmentations is with a custom made implant from a 3D CT scan. It is critically important to cover a large surface area of the skull in a smooth and confluent manner to the bone which can only be done with a preoperatively done design based on the patient’s actual anatomy. Bone cements are a poor substitute for aesthetic skull augmentation when any significant amount of surface area coverage or volume increase is needed.
Because 3D custom skull implants are capable of covering large areas of the bone and can add hundreds of ccs of volume, the limiting factor becomes how much can the scalp stretch to accommodate it. The scalp is not limitless in how much it can stretch from an expansile force underneath it. While every scalp is different my extensive experience indicates that 10mm to 12 mms of central projection height increase with a volume of around 150ccs is the limit in a single intervention. (this will, of course, vary greatly depend on the size of the person and the thickness of their scalp)
It is for this reason that large skull augmentations require a two-stage approach, an initial scalp tissue expander followed later by the placement of the implant. For those patients who seek large skull augmentations they usually choose this treatment and they know so right from the beginning. But the concept of a two-stage skull augmentation approach is not appealing for many patients, particularly those who are uncertain if they really need that much volume or want to put in that such ‘effort’. They may opt for. an immediate implant insertion and hope that meets their aesthetic goals or at least comes close.
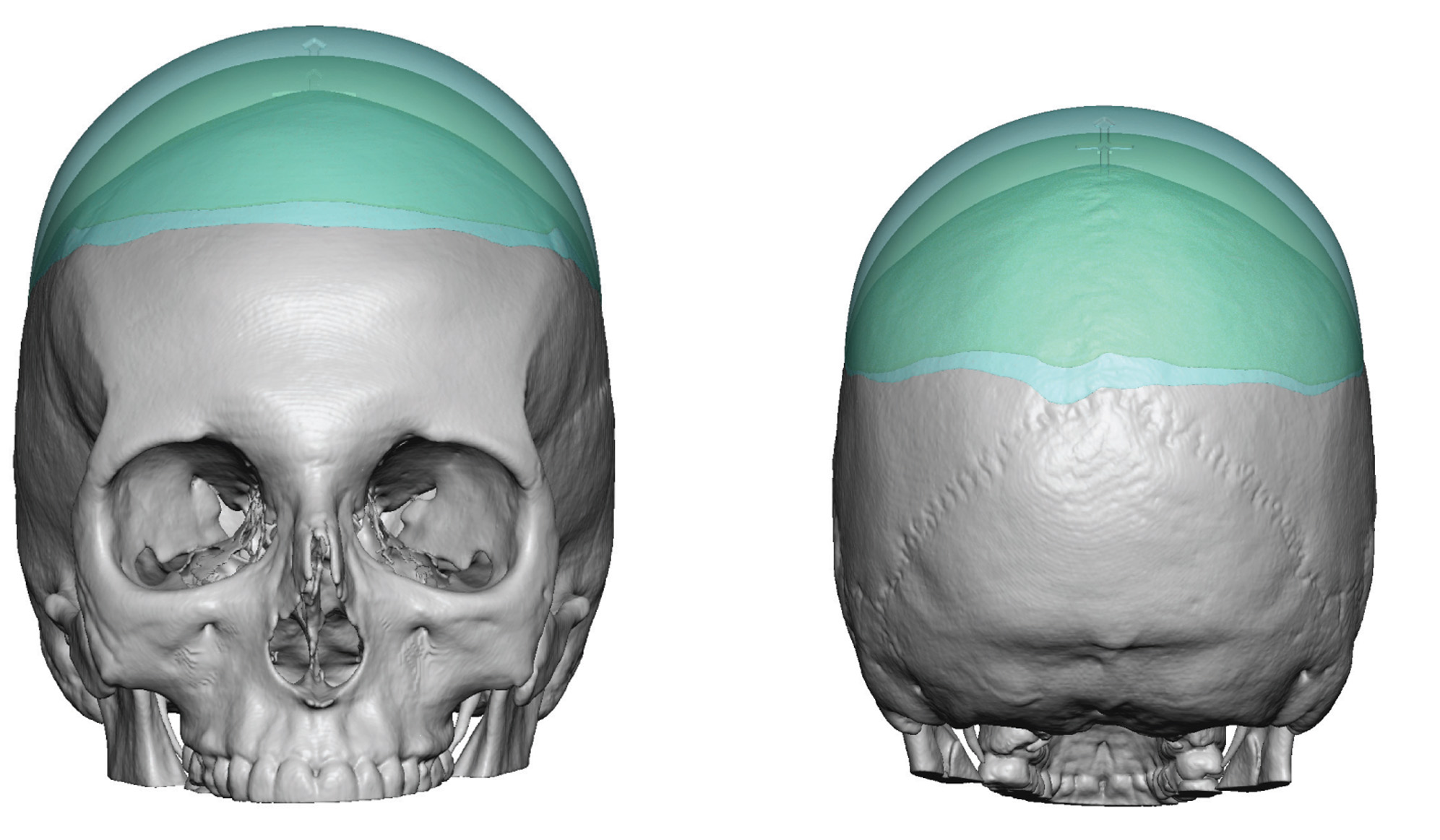
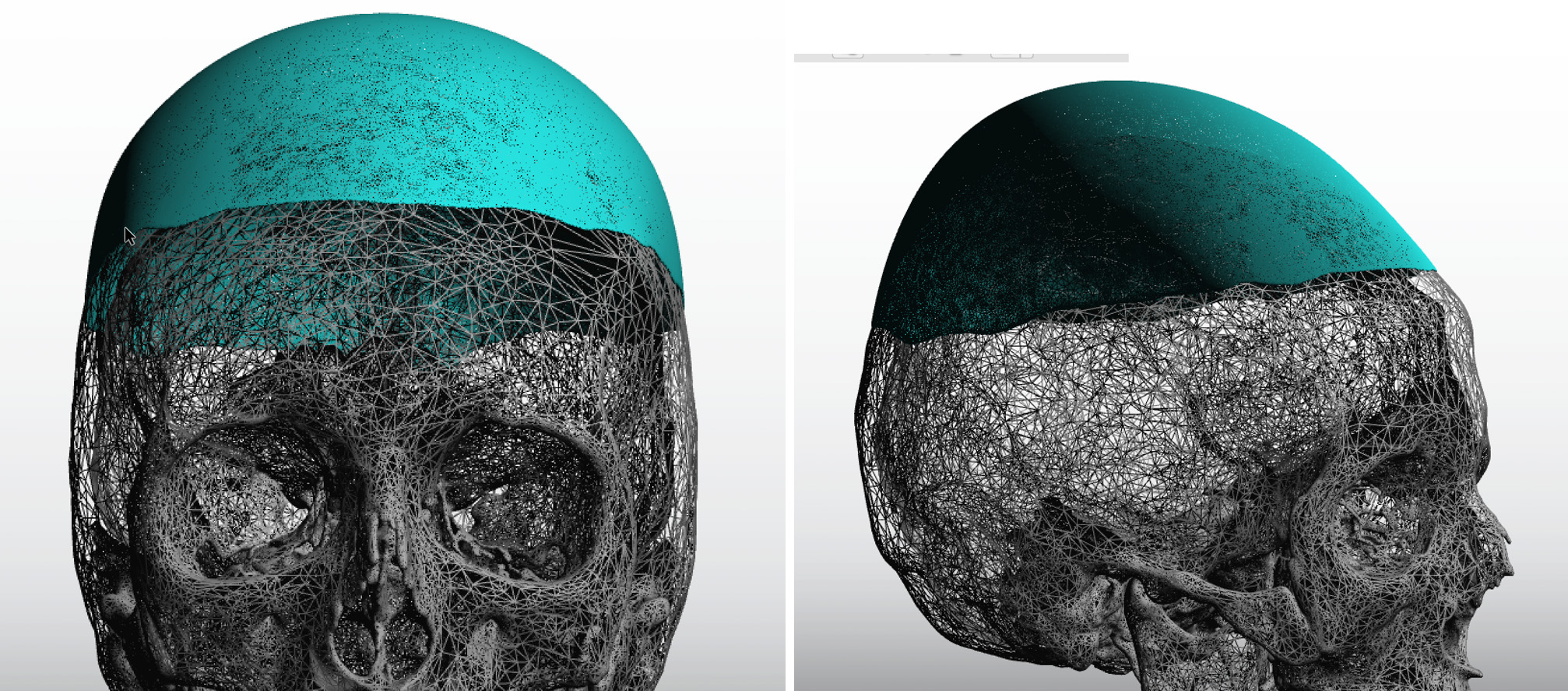
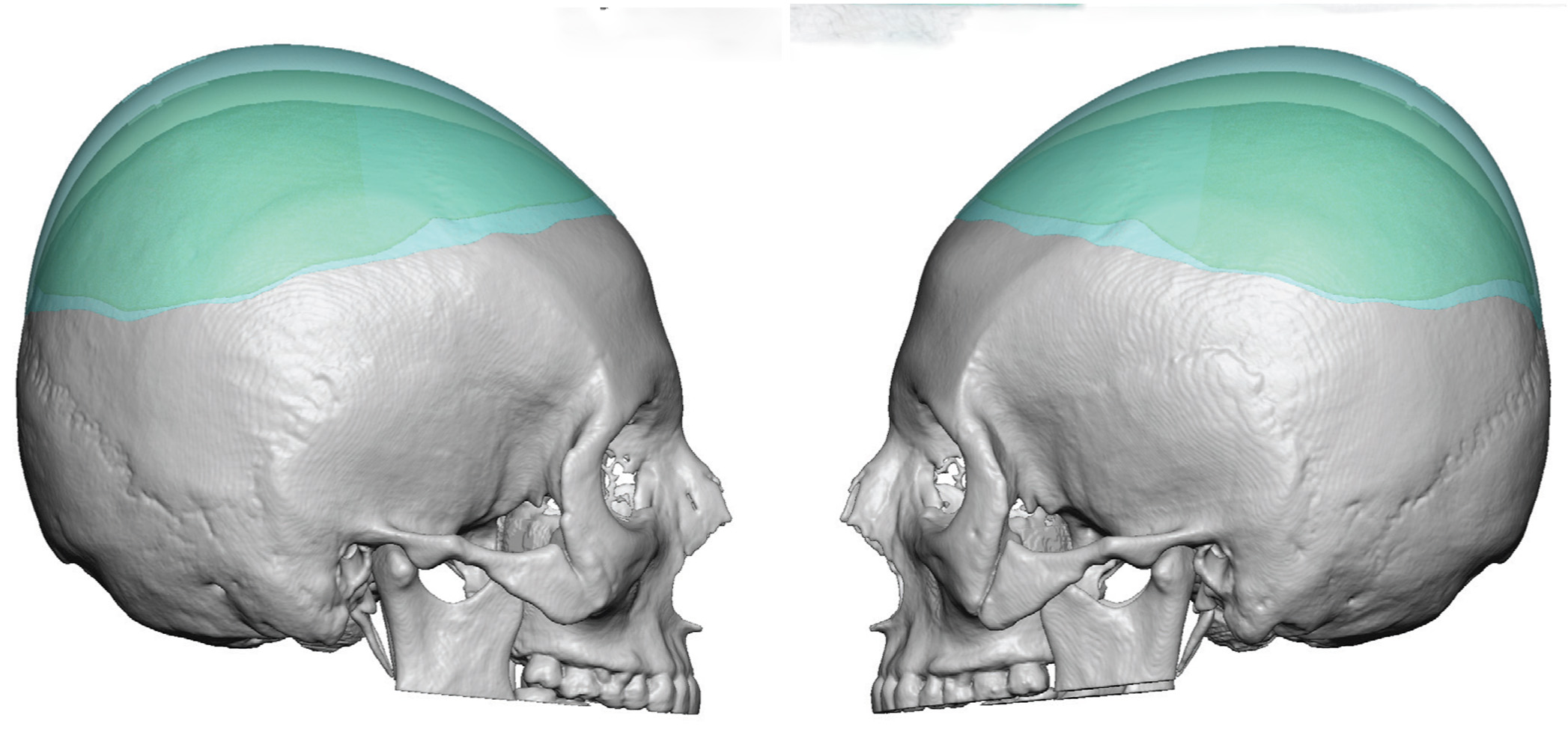 Case Study: This 35 year-old female had a custom skull implant placed for crown augmentation two years previously. While this provided good improvement she eventually decided she wanted more height and opted for a larger implant. Her new implant was designed off of her original 3 CT scan and implant design. The maximal central projection was increased from 8mm to 16ms with corresponding increases in the width down into the upper temporal regions to maintain a proper shape .
Case Study: This 35 year-old female had a custom skull implant placed for crown augmentation two years previously. While this provided good improvement she eventually decided she wanted more height and opted for a larger implant. Her new implant was designed off of her original 3 CT scan and implant design. The maximal central projection was increased from 8mm to 16ms with corresponding increases in the width down into the upper temporal regions to maintain a proper shape .
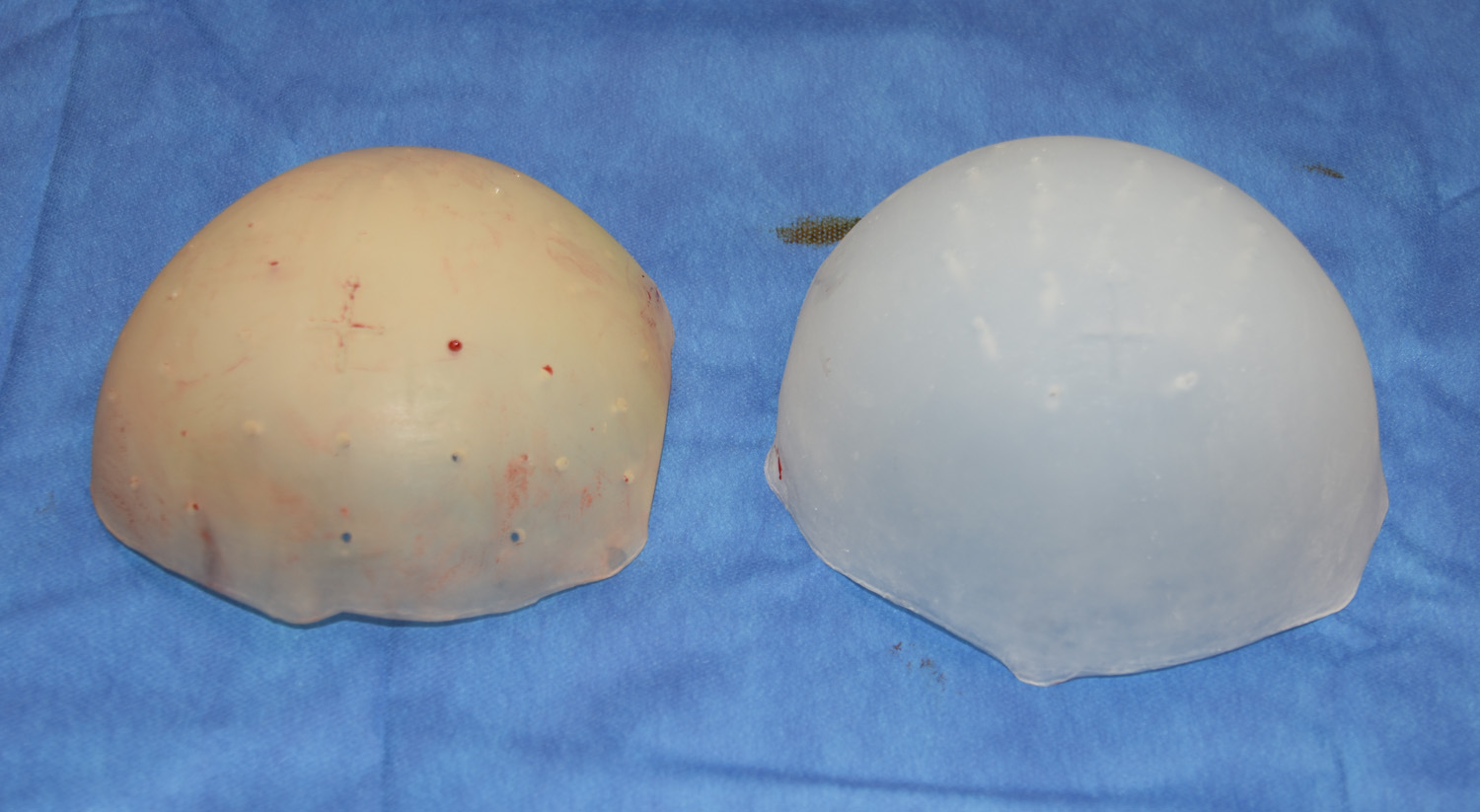 In surgery her existing skull implant was removed and replaced with the new larger one. The scalp was able to be successfully closed over it by partial capsulotomes around the base of the implant capsule. The tightness of the scalp closure required metal clips for the skin rather than the traditional 5-0 plain sutures that I typically use. A side by side comparison of the removed vs new implant showed the differences in their size.
In surgery her existing skull implant was removed and replaced with the new larger one. The scalp was able to be successfully closed over it by partial capsulotomes around the base of the implant capsule. The tightness of the scalp closure required metal clips for the skin rather than the traditional 5-0 plain sutures that I typically use. A side by side comparison of the removed vs new implant showed the differences in their size.
 Deciding to replace an existing skull implant for a larger one can be successfully done with size/volumetric increase of 50% to 100%. In essence the first implant has acted like a tissue expander as now would anticipate. This is encouraging information for those patients who undergo an immediate skull implant but wonder that if it does not meet their head shape goals as to what their future options would be.
Deciding to replace an existing skull implant for a larger one can be successfully done with size/volumetric increase of 50% to 100%. In essence the first implant has acted like a tissue expander as now would anticipate. This is encouraging information for those patients who undergo an immediate skull implant but wonder that if it does not meet their head shape goals as to what their future options would be.
Highlights:
1) Large skull augmentations require a two stage approach to ensure adequate scalp coverage.
2) One version of a two stage approach is a delayed approach using two separate skull implants.
3) The placement of a second stage skull implant usually allows for a doubling of augmentation volume.
Dr. Barry Eppley
Indianapolis, Indiana