

Background: The shape of the back of the head is affected by many factors. While flatness and asymmetries are well known to be caused by intrauterine and postnatal head positioning, limiting growth expansions in the compressed area, the origins of bony protrusions are less clear. In a study published in the Journal of Craniofacial Surgery in 2013, occipital protrusions or ‘very round heads’ were seen in only 3% of men studied. Excessive flatness was far more common at over 15%.
Regardless of its percentage of occurrence to those affected a excessive roundness of the back of head is aesthetically bothersome. Such occipital protrusions can be reduced and the extent of its effect is based on the thickness of the bone. Specifically it is based on the thickness of the other table of the skull. This is the layer of skull bone that can be safely removed without undue bleeding or risking making the skull too thin.
 The skull is a flat bone (like the sternum and ribs) that forms boundaries of body cavities. (in this case the brain) It is a sandwich of spongy bone between two layers of compact bone. Moving the outer layer can always done and represents about 1/3 of the skull’s thickness. What reductive effect that may have is around 7mms, which may not sound like much, until one considers the broader surface of bone that is removed. Whether this is enough for any patient must be considered on an individual patient basis.
The skull is a flat bone (like the sternum and ribs) that forms boundaries of body cavities. (in this case the brain) It is a sandwich of spongy bone between two layers of compact bone. Moving the outer layer can always done and represents about 1/3 of the skull’s thickness. What reductive effect that may have is around 7mms, which may not sound like much, until one considers the broader surface of bone that is removed. Whether this is enough for any patient must be considered on an individual patient basis.
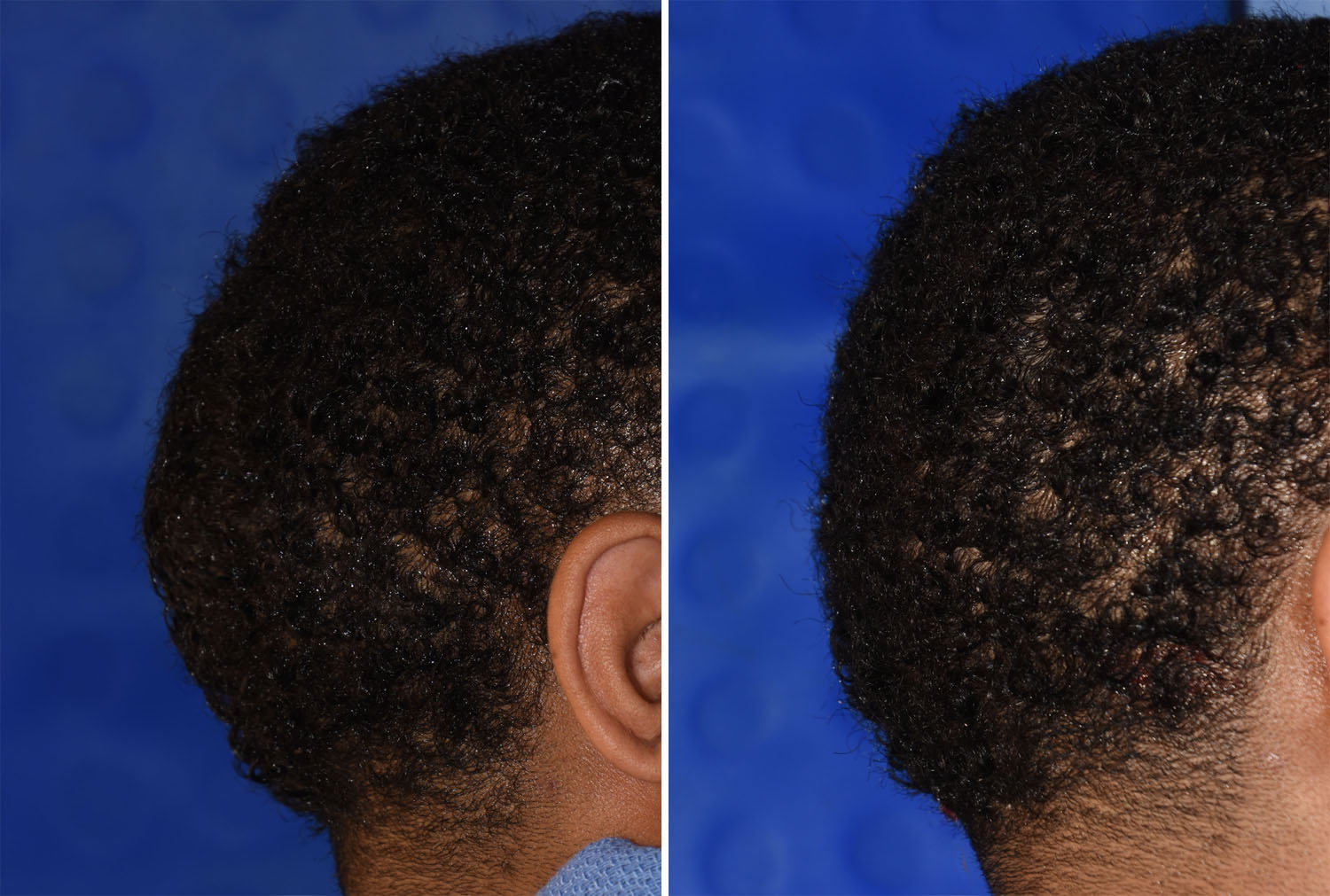
Case Study: This young male was bothered by the protrusion that jutted out from teh back of his head. It was about the size of a hand in shape (my hand) and was located over the central or central-low occipital skull position.
 Under general anesthesia and in the prone position, a wavy 9cm long scalp incision was made in a horizontal orientation over the mid-occipital region. To ensure evenness in bone removal, a central vertical and horizontal line of bone removal was first done down to the desired depth of removal. This created four quadrants of bone which could be individually removed mindful of its depth and curvature outward to the top, sides and bottom. This allows the entire outer cortical table of bone to be removed, like harvesting split thickness cranial bone grafts.
Under general anesthesia and in the prone position, a wavy 9cm long scalp incision was made in a horizontal orientation over the mid-occipital region. To ensure evenness in bone removal, a central vertical and horizontal line of bone removal was first done down to the desired depth of removal. This created four quadrants of bone which could be individually removed mindful of its depth and curvature outward to the top, sides and bottom. This allows the entire outer cortical table of bone to be removed, like harvesting split thickness cranial bone grafts.
 The grid technique of skull reduction allows for a regimented approach to reducing a large bone surface and to do so in an even fashion. It allows the most common area for skull reduction, the back of the head, to be satisfactorily reduced for patient bothered by mild to moderate occipital skull protrusions.
The grid technique of skull reduction allows for a regimented approach to reducing a large bone surface and to do so in an even fashion. It allows the most common area for skull reduction, the back of the head, to be satisfactorily reduced for patient bothered by mild to moderate occipital skull protrusions.
Highlights:
1) Occipital skull protrusions can be reduced twosome degree based on the thickness of the skull bone.
2) The skull reduction of the back of the head is approached through a horizontal wavy scalp incision of around 9 cms.
3) A grid reduction technique is used to remove the outer cortical layer of the skull.
Dr. Barry Eppley
Indianapolis, Indiana