

Background: The perception of excessive head width is usually seen as a convex shape to the side of the head above the ears. This makes the side of the head bow out and gives the overall head shape more of a ‘lightbulb’ appearance particularly when the lower facial features are smaller and more narrow. There may also be other aesthetic issues besides its appearance such as having trouble wearing glasses or hats that feel too tight.
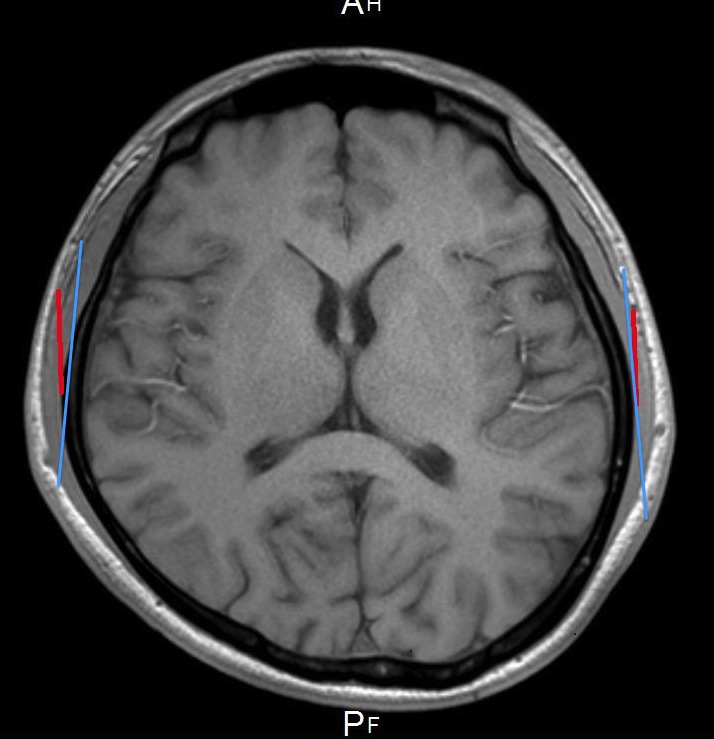 The width of the head is comprised of the temporal bone and muscles. The widest part of the side of the head is the posterior temporal area above the ears. While it is commonly perceived that any such bowing is largely due to the thickness of the posterior portion of the temporal bone, this is an anatomic inaccuracy. While the bone does make a significant contribution, the thickness of the posterior belly of the temporal muscle makes up at least 50% of its width. This can be appreciated by looking at coronal images of a CT scan where the thickness of the muscle can be better appreciated. In my experience it usually measures anywhere from 7 to 9mms in thickness above the ear.
The width of the head is comprised of the temporal bone and muscles. The widest part of the side of the head is the posterior temporal area above the ears. While it is commonly perceived that any such bowing is largely due to the thickness of the posterior portion of the temporal bone, this is an anatomic inaccuracy. While the bone does make a significant contribution, the thickness of the posterior belly of the temporal muscle makes up at least 50% of its width. This can be appreciated by looking at coronal images of a CT scan where the thickness of the muscle can be better appreciated. In my experience it usually measures anywhere from 7 to 9mms in thickness above the ear.
Removal of the posterior portion of the temporal muscle can create a very visible reduction in head width. I have performed it many times and have come to appreciate both its effectiveness and safety. Removal of this portion of the temporal muscle is not associated with any chewing or mouth opening difficulties. Surprisingly most patients do not even have any stiffness or soreness of mouth opening even the day after surgery.
Since a significant percent of patients seeking head width reduction are men, often with close cropped hair or a shaved head, the relevance of any visible scars from this procedure is an important aesthetic issue.
Case Study: This very young male had long been bothered by the shape of his head. He felt it bulged out at the sides and make his head too round for the shape of his face.

 Under general anesthesia, the posterior temporal zone of muscle removal was marked out. Through a postauricular incision and in a subfascial plane, the entire posterior portion of the temporal muscle was removed. The overlying deep temporal fascia was left intact. The incision behind the ear was closed with dissolveable sutures.
Under general anesthesia, the posterior temporal zone of muscle removal was marked out. Through a postauricular incision and in a subfascial plane, the entire posterior portion of the temporal muscle was removed. The overlying deep temporal fascia was left intact. The incision behind the ear was closed with dissolveable sutures.



 His immediate surgery results (one day later) showed a visible reduction in the width of his head. Further swelling reduction would be expected to enhance the result over the next month. He had no chewing pain or mouth opening restrictions. He had some ear swelling which made his ears protrude slightly more than they did before surgery. This is a self-solving issue as the swelling subsides.
His immediate surgery results (one day later) showed a visible reduction in the width of his head. Further swelling reduction would be expected to enhance the result over the next month. He had no chewing pain or mouth opening restrictions. He had some ear swelling which made his ears protrude slightly more than they did before surgery. This is a self-solving issue as the swelling subsides.
Head width reduction by posterior temporal muscle removal can be done successfully without visible scarring in the temporal region. Two key surgical techniques are keeping the overlying fascia intact and re-establishing the attachments of the ear to the side of the head during closure.
Highlights:
1) Excessive head width often refers to a fullness or convexity above the ears.
2) A substantial amount of excessive head width is due to the thickness of the posterior temporal muscle
3) Head width reduction can be achieved through removal of the posterior temporal muscle through an incision limited to behind the ear.
Dr. Barry Eppley
Indianapolis, Indiana