

Background: Early cranial vault surgery for a variety of congenital craniosynostosis disorders has been done for over thirty years. Such surgery is done at an early because the bone is thin enough to be able to be removed and reshaped and the dura covering of the brain has some remaining osteogenic potential. This means that any defects of the skull that result from the reconstruction (and there are often many of them) is able to heal and fill in with bone due to the underlying dura.
But despite the osteogenic potential of the infant’s dura, larger bone defects may not fully heal in after cranial vault reconstruction. While very small full-thickness bone defects may be acceptable to be left alone, large skull defects require secondary reconstruction.
The methods of secondary skull reconstruction in children come down to using the patient’s own bone or using a synthetic material. If the child is old enough a skull bone graft can be harvested in a split cranial bone graft technique but this potentially occurs creating another skull defect in another location. Alternatively the most common implant material in children would be hydroxyapatite cement. This liquid and powder mixture creates a putty which is applied and shaped to the defect and then slowed to set or cure. This setting process can be affected by sitting directly in top of a pulsating dural surface.
Case Study: This older male child has a unilateral coronal craniosynotsosis repair as an infant at 8 months of age. By age 6 it could be felt and seen by x-rays that he had a large remaining bone defect behind the frontal bone flap that was advanced on the affected side.
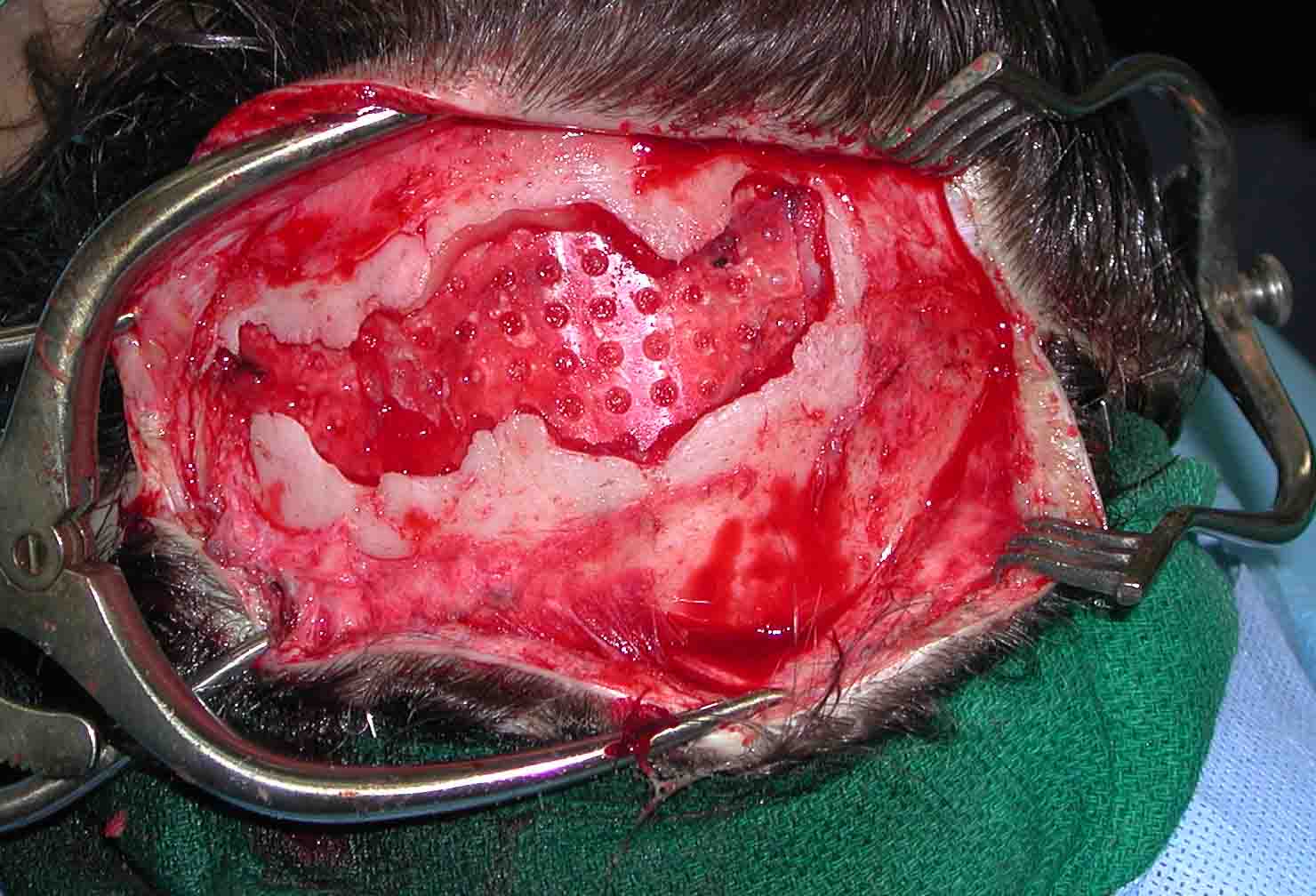
 Under general anesthesia his scalp scar from his original coronal scalp incision was open and the bone defect exposed. The duras was dissected off of the bone edges and a 1mm thick resorbable panel (Lactosorb) was placed under the bone edges and locked it in to position between the dura and the bone edges to form the floor for the reconstruction. Using 20 grams of hydroxyapatite cement (Mimix), the bone defect was filled into and the cement allowed to set creating a stable and complete skull reconstruction.
Under general anesthesia his scalp scar from his original coronal scalp incision was open and the bone defect exposed. The duras was dissected off of the bone edges and a 1mm thick resorbable panel (Lactosorb) was placed under the bone edges and locked it in to position between the dura and the bone edges to form the floor for the reconstruction. Using 20 grams of hydroxyapatite cement (Mimix), the bone defect was filled into and the cement allowed to set creating a stable and complete skull reconstruction.
Hydroxyapatite cement offers the most natural of all synthetic materials for skull reconstruction. It is usually used for partial thickness skull defects because its putty-like form when it is mixed requites a stable background on which to be molded, shaped and then allowed to set. But in full-thickness skull defects a stable background can be made from a variety of materials. But in children the use of a resorbable backing, which has a function in the short-term and is resorbed in the long-run, seems a logical choice.
Highlights:
1) Early cranial vault reconstruction for craniosynostosis can lead to secondary bone defect sites behind the advanced bone flaps.
2) Reconstructing full thickness skull bone defects can be done using hydroxyapatite cement.
3) The floor of skull bone defects can be made using resorbable mesh panels so the bone cements has a solid backing on which to set and cure.
Dr. Barry Eppley
Indianapolis, Indiana