

Background: In chin augmentation treatment options consist of either an implant placed on top of the bone or to move the chin bone forward. (sliding genioplasty) Often it is perceived that these two chin enhancement methods are competitive options but that is not really the case. Conversely each method has distinct advantages and disadvantages which must be considered on an individual case basis.
The sliding genioplasty is a chin bone procedure that has been around for a long time. While it has evolved in its technique over the years from its namesake (it really doesn’t slide forward along the bone cut as it has been historically described), it does move the edge of the chin bone forward. What is often not appreciated about the procedure is that it is really a pedicled myo-osseous bone flap. Its posterior preserved muscle attachments is how the bone survives after it is cut off from the upper chin bone. As a result of these attachments the geniohyoid and genioglossus muscles are pulled forward which can have a positive neck contouring (lifting) effect.
It is my opinion that in severely short chins (greater than 10mm to 12mms horizontal deficiency) an implant is not the best long chin augmentation procedure for some patients. There are other anatomic issues around the chin that need to be improved which an implant can not do. At the very least if the sliding genioplasty is still aesthetically insufficient, it serves as an improved foundation for an implant to be done later.
Case Study: This young male had a severe chin deficiency that ensures as 18mm short by the classic vertical line down from the lip measurement. He was also vertically short in wore facial height as is often common in severe lower jaw deficiency. However he had an orthodontically corrected occlusion which negated the possibility of total lower jaw advancement surgery.
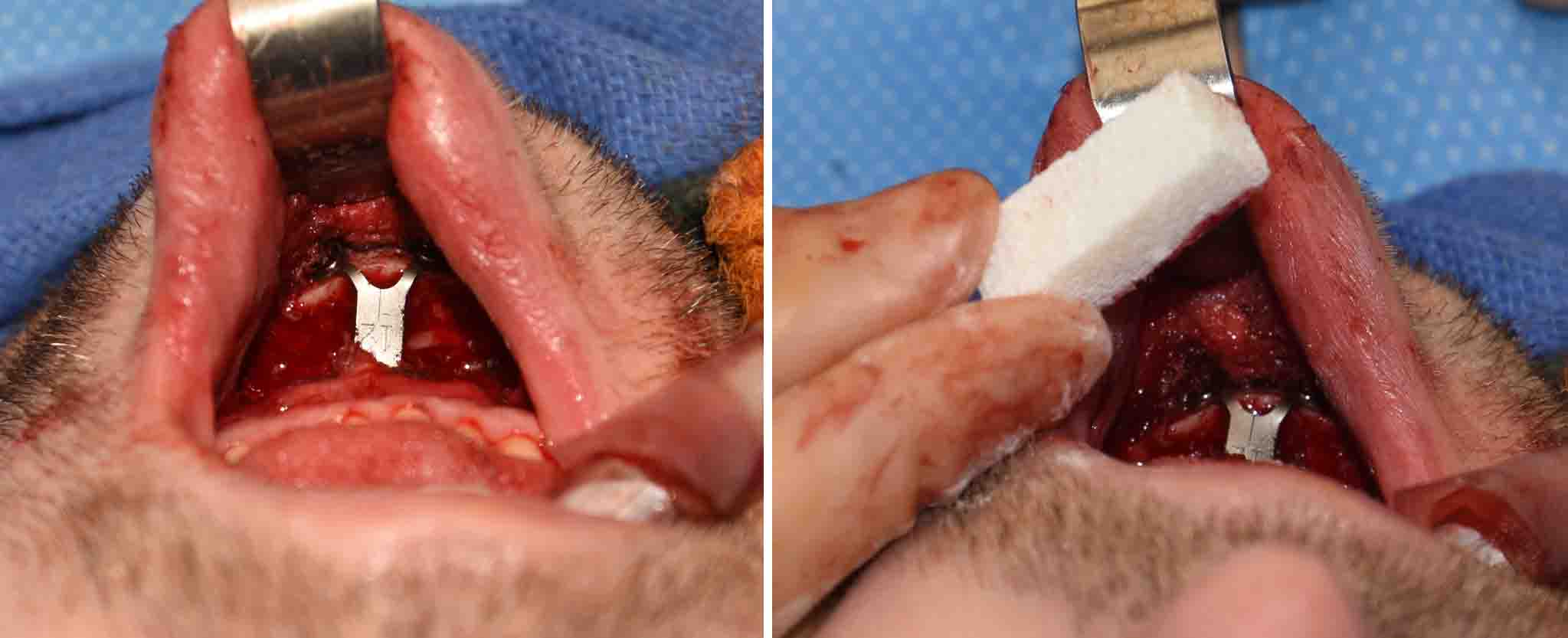
 Under general anesthesia an intraoral sliding genioplasty was performed with a combined horizontal projection and vertical lengthening effect. The downfractured chin bone segment was secured by a 12mm chin plate that was bent downward to add 4mms of vertical lengthening as well. This left a large bone gap anterior in the ‘open wdge’ area which was graft using an allograft bone block (cadaveric bone) that was sectioned and shared to serve as a wedge between the upper and lower bone segments.
Under general anesthesia an intraoral sliding genioplasty was performed with a combined horizontal projection and vertical lengthening effect. The downfractured chin bone segment was secured by a 12mm chin plate that was bent downward to add 4mms of vertical lengthening as well. This left a large bone gap anterior in the ‘open wdge’ area which was graft using an allograft bone block (cadaveric bone) that was sectioned and shared to serve as a wedge between the upper and lower bone segments.
 Large sliding genioplasty movements leave significant bone gaps. Even though there is a central rigid plate holding the respositioned bone segment in the desired position, that does not ensure that it will heal completely by bony union. To help expedite more complete healing of the bone segments, an interpositional bone graft is helpful. While using the patient’s own bone is ideal, few patients want to have a bone graft harvest for a chin procedure. Allograft bone is ideal for use in a non-load bearing area of the lower jaw. It can be easily shaped to create a snug fit into any such shaped bone gaps.
Large sliding genioplasty movements leave significant bone gaps. Even though there is a central rigid plate holding the respositioned bone segment in the desired position, that does not ensure that it will heal completely by bony union. To help expedite more complete healing of the bone segments, an interpositional bone graft is helpful. While using the patient’s own bone is ideal, few patients want to have a bone graft harvest for a chin procedure. Allograft bone is ideal for use in a non-load bearing area of the lower jaw. It can be easily shaped to create a snug fit into any such shaped bone gaps.
Case Highlights:
1) A sliding genioplasty is the autologous option in chin augmentation
2) In severely short chins, a sliding genioplasty is preferred over an implant as it establishes a solid bony base and pulls certain neck muscle forward.
3) In large sliding genioplasty advancements, an interpositional graft is helpful for both long-term healing and bony stability.
Dr. Barry Eppley
Indianapolis, Indiana