

Background: Skull deformities of the back of the head are very common. It is probably the one skull area that has the greatest incidence of shape distortions. This likely occurs because it is the most exposed skull area to deformational force both in utero and after birth due to fetal and neonatal positioning. Thus flat spots on the back of the head are common and occur in a wide variety of locations and extent.
Aesthetic reconstruction of the flat back of the head can be done by a variety of implant techniques. The most common skull reshaping technique today is the use of a custom occipital implant made from the patient’s 3D CT scan. This works well for large flat spots on the back of the head (brachycephaly) as well as those that are associated with some significant asymmetry. (plagiocephaly)
While a custom implant would also work well for smaller flat spots, the cost and the time of manufacture for some patients may exclude this as a treatment option. The use of traditional cranioplasty bone cements, such as PMMA, provide an immediate and relatively low cost skull implant option that can be done immediately and with good long-term results. The key to its aesthetic use is a small incision and getting good shaping of the material as it cures.
Case Study: This 31 year male was bothered by a very discrete flat spot on the central area of the back of his head. It created a sharp step-off at the very end of the sagittal skull area, creating a 90 degree angle between the top of the head and that of the back of the head. Due to cost and being from out of the country, a custom implants was not an implant option.
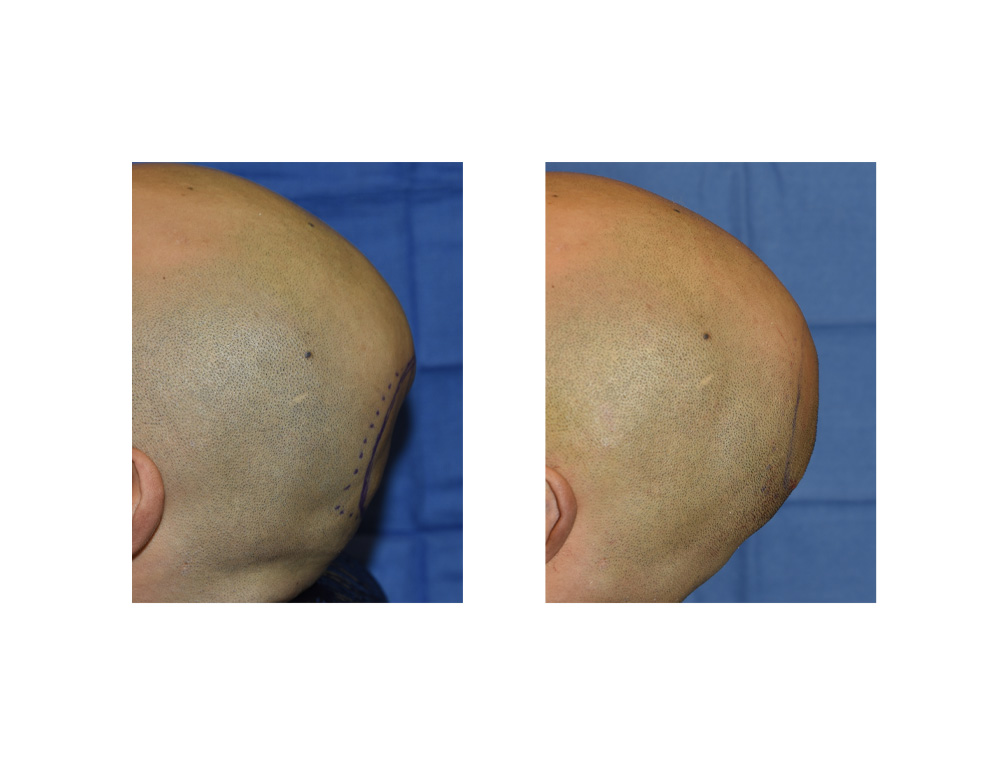
 Under general anesthesia in the beach chair position, a 5.5 cm horizontal scalp incision was made at the bottom end of the flat spot. Through this incision antibiotic impregnated PMMA cranioplasty bone cement was mixed and 40 grams of it as introduced under the widely raised subperiosteal scalp flap over the flat spot. The cement was shaped externally and allowed to set with a focus of smooth edges around the cement’s perimeter. A good intraoperative back of the head contour was obtained.
Under general anesthesia in the beach chair position, a 5.5 cm horizontal scalp incision was made at the bottom end of the flat spot. Through this incision antibiotic impregnated PMMA cranioplasty bone cement was mixed and 40 grams of it as introduced under the widely raised subperiosteal scalp flap over the flat spot. The cement was shaped externally and allowed to set with a focus of smooth edges around the cement’s perimeter. A good intraoperative back of the head contour was obtained.

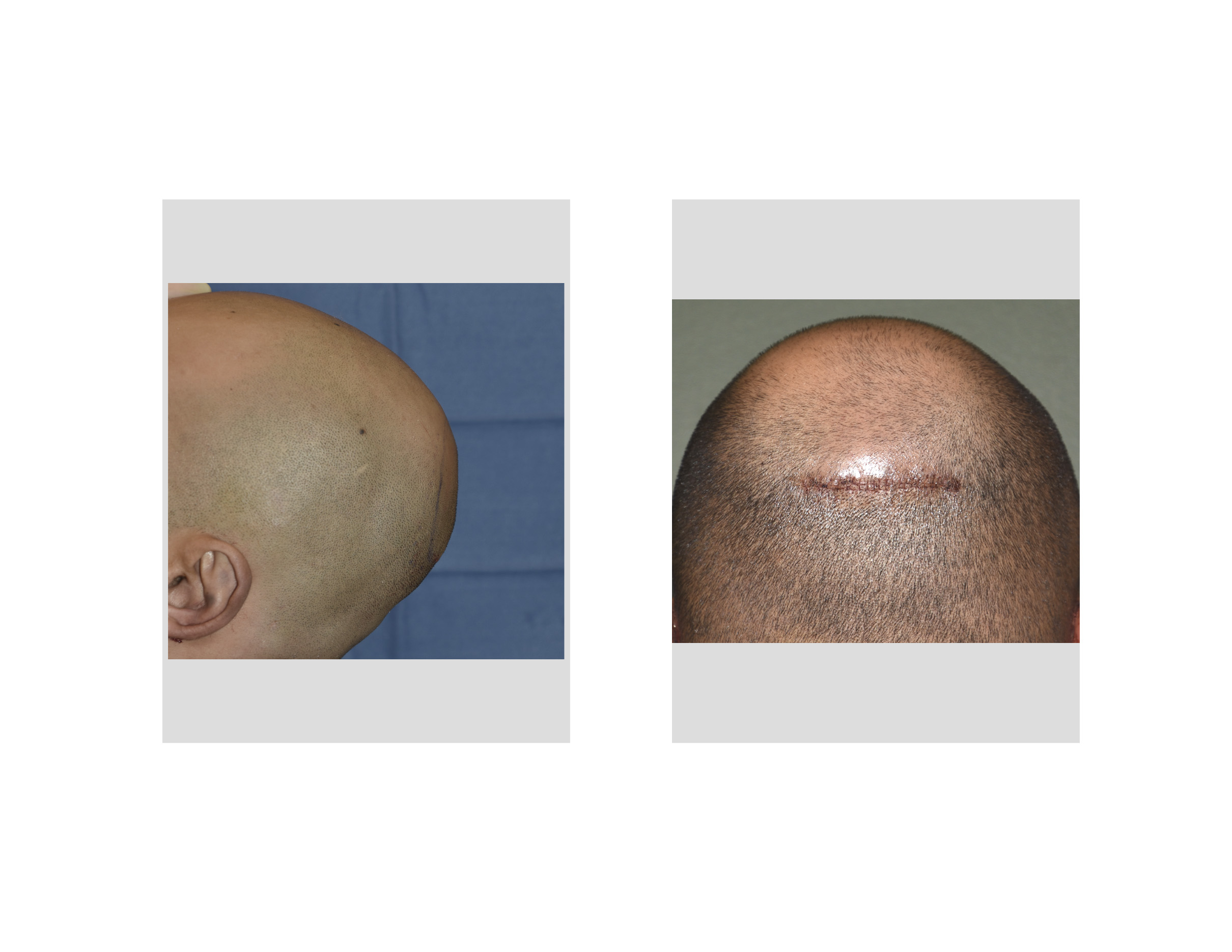
 At one week after surgery both profile views of the back of his head showed good shape improvement. It takes about three more weeks for all scalp swelling to completely resolve. He had simultaneous otoplasty procedures as well hence the bruising around his ears.
At one week after surgery both profile views of the back of his head showed good shape improvement. It takes about three more weeks for all scalp swelling to completely resolve. He had simultaneous otoplasty procedures as well hence the bruising around his ears.
A minimal incision PMMA bone cement cranioplasty relies on shaping the material in a blind fashion once placed into the created pocket. There is no forgiveness for any edge transition or step off problems between the cement and the bone since is no way to access them for adjustment (burring reduction) through such a small incision. This is a learned cranioplasty techique that takes a lot of experience to do consistently well.
Highlights:
- Defects of the back of head (occiput) occur in a wide variety of shapes but a flat spot is often the predominant problem.
- The use of PMM bone cement can be used for selective flat spots on the back of the head.
- A small or minimal incision approach can be done for a PMMA bone cement occipital cranioplasty but placing and shaping the cement is a learned skill.
Dr. Barry Eppley
Indianapolis, Indiana