

Background: Aesthetic skull concerns present in a variety of shapes, depressions, bumps and prominences. Some are due to birth defects and trauma but the vast majority are due to genetics and simply how the skull has developed for unknown reasons. But some aesthetic skull anomalies are there for an actual anatomic reason.
 Such is the case of the prominent nuchal ridge on the back of the head. It exists as an attachment area for various neck muscles. While normally barely visible, even in a shaved head, it can become very visible. If the nuchal ridge is thick enough it will protrude out creating an abnormal bulge. This will extend entirely across the back of the head but is usually thickest in the middle. It can be obvious even in close cropped hairstyles and can be aesthetic concern for some men. (I have never seen it yet in a woman)
Such is the case of the prominent nuchal ridge on the back of the head. It exists as an attachment area for various neck muscles. While normally barely visible, even in a shaved head, it can become very visible. If the nuchal ridge is thick enough it will protrude out creating an abnormal bulge. This will extend entirely across the back of the head but is usually thickest in the middle. It can be obvious even in close cropped hairstyles and can be aesthetic concern for some men. (I have never seen it yet in a woman)
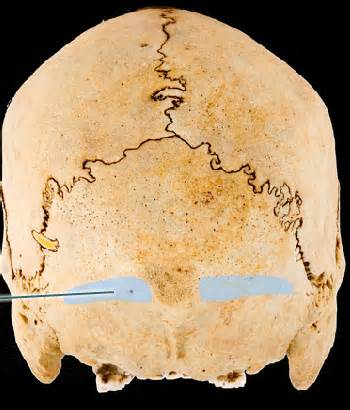
Calling the raised bone ridge across the back of the skull a single nuchal ridge or crest is a bit oversimplified. The nuchal ridge per se is really a set of four curved lines on the occipital bone. The highest nuchal line is where the galea of the scalp attaches and is a barely visible bone line. Below it lies the superior nuchal line, which is what is commonly called the ridge, because it is more prominent because of its muscular attachments. (splenius capitis, occipitalis and trapezius muscles) Below this lies the very faint median and inferior nuchal lines to which muscles also attach and are closer to the foramen magnum.
Why some nuchal ridges are very prominent and others are not is not precisely known. It is assumed that it is present because of very strong muscle attachments. Using the form follows function theory, one can assume those with larger nuchal ridges have very thick and strong muscular attachments. This may also account for why some patients with prominent nuchal ridges have occipital migraines/headaches. (personal observation)
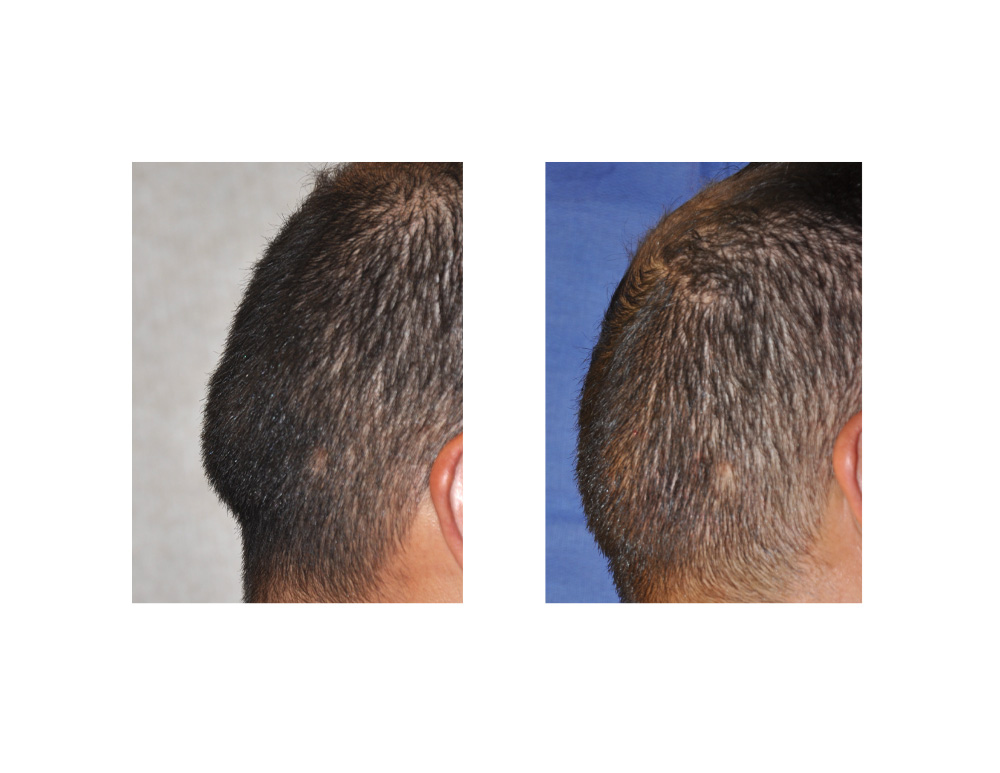
Case Study: This 43 year-old male presented with a prominent nuchal ridge that was aesthetically bothersome. It bulged out at the bottom of the back of his head. It was thickest in the middle and tapered down from the center on each side. He also had a history of intermittent occipital-based headaches and a tight neck.
 Under general anesthesia in the prone position and without shaving any hair, a 5 cm long horizontal incision was made parallel to it. The raised ridge was dissected out at the subperiosteal level, releasing the muscle attachments at the bottom side of it. A handpiece and burr was used to completely flatten the ridge from side to side, reducing it by as much as 9mm in the middle. Bone wax was used to fill any bleeding bone holes. Closure was done in multiple layers with small resorbable sutures for the skin.
Under general anesthesia in the prone position and without shaving any hair, a 5 cm long horizontal incision was made parallel to it. The raised ridge was dissected out at the subperiosteal level, releasing the muscle attachments at the bottom side of it. A handpiece and burr was used to completely flatten the ridge from side to side, reducing it by as much as 9mm in the middle. Bone wax was used to fill any bleeding bone holes. Closure was done in multiple layers with small resorbable sutures for the skin.
 Nuchal ridge reduction produces an immediate and aesthetically satisfying occipital skull reshaping procedure. Recovery is quick and patients do not complain of much discomfort other than some initial upper neck soreness. It remains to be seen whether such bone reduction and muscle release result in headache improvement.
Nuchal ridge reduction produces an immediate and aesthetically satisfying occipital skull reshaping procedure. Recovery is quick and patients do not complain of much discomfort other than some initial upper neck soreness. It remains to be seen whether such bone reduction and muscle release result in headache improvement.
Case Highlights:
1) One type of occipital skull deformity is that of the prominent nuchal ridge which forms a raised horizontal ridge across the back of the head.
2) The prominent nuchal ridge should not be confused with the occipital knob which is a raised button of bone at the center of the nuchal ridge.
3) Nuchal ridge reduction is done through a small horizontal incision over the central part of it.
4) Some patients with a prominent nuchal ridge have intermittent occipital headaches due to tight neck muscle attachments.
Dr. Barry Eppley
Indianapolis, Indiana