

Background: The most common major aesthetic ear surgery is the setback otoplasty. With a long surgical history numerous methods have been described for setting back the protruding ear and decreasing the auriculocephalic angle. (bring the ear back closer to the head) The fundamental concept is that the ear cartilages have to be manipulated either by suture reshaping with or without cartilage weakening and/or affixing the cartilages to the mastoid fascia.
No matter the method used, changing the shape of the ear and its auriculocephalic angle is an intraoperative judgment as to the amount of aesthetic change needed. Otoplasty is not an exact science. The most common aesthetic complications with otoplasty are over correction and asymmetry with asymmetry being more common than overcorrection.
If caught early, the overcorrect otoplasty can be improved by simple suture release and/or replacement. But since sufficiency scar tissues has formed and the cartilage has lost its memory (months later), suture methods alone will not be adequate.
Case Presentation: This young man had an otoplasty done years ago with the right side having a good result but left side being pulled back too far. The left ear showed the absence of a helical rim in the front view with only the antihelical rim being seen. He achieved his desired effect by pushing out from behind the ear in its central third.
 Under local anesthesia, his original postauricular incision was opened the cartilages released by scar tissue removal and cartilage scoring. The using a bent 1mm mesh fixation plate that was cut to 90 degrees, it was inserted and stabilized to the back side of the anti helix cartilage (superiorly) and the mastoid fascia (inferiorly) with restorable sutures.
Under local anesthesia, his original postauricular incision was opened the cartilages released by scar tissue removal and cartilage scoring. The using a bent 1mm mesh fixation plate that was cut to 90 degrees, it was inserted and stabilized to the back side of the anti helix cartilage (superiorly) and the mastoid fascia (inferiorly) with restorable sutures.
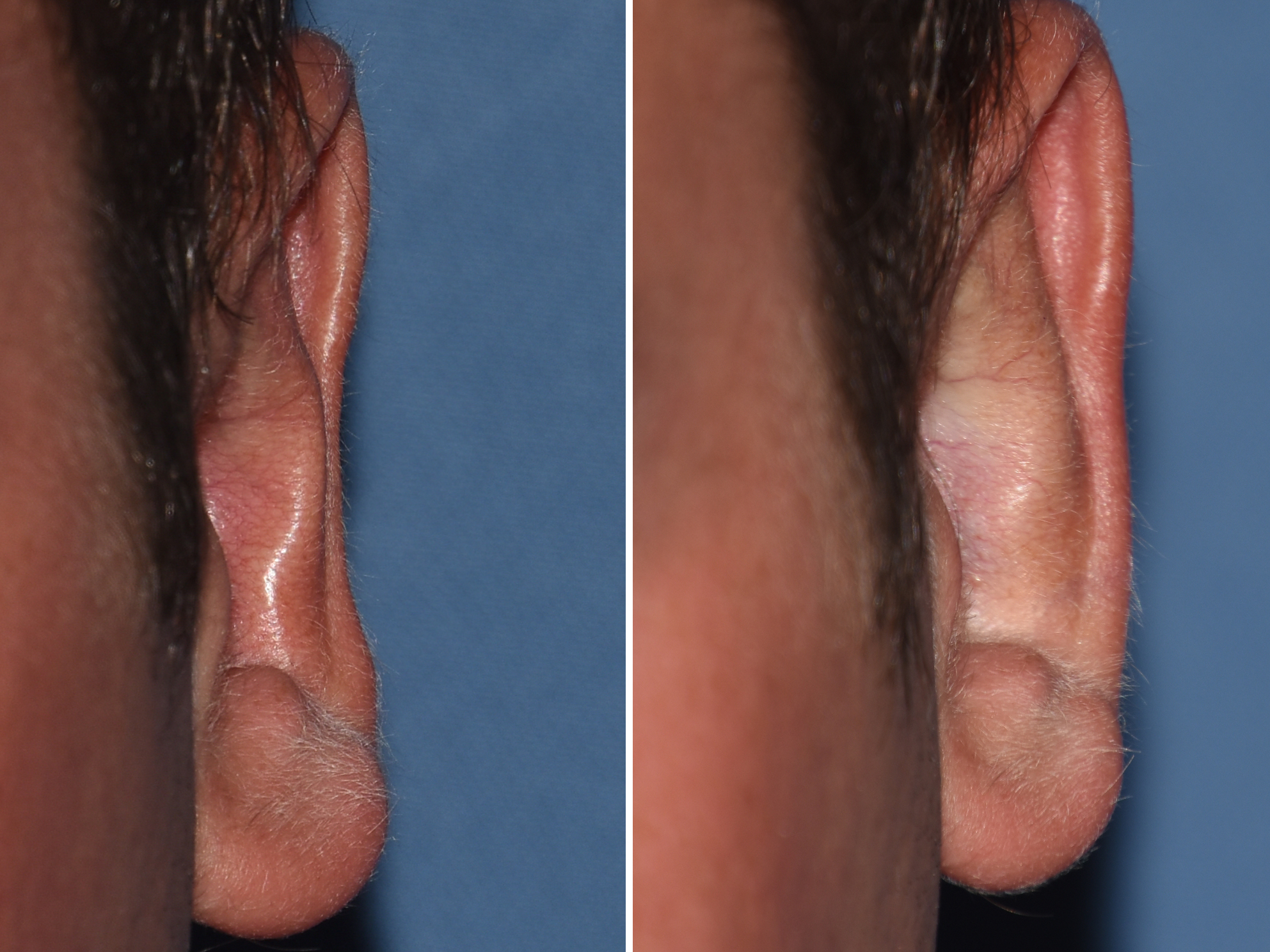 The effect of the otoplasty reversal procedure was immediate with the helical rim profile being now seen above that of the anti helical rim. Options to stabilize or hold the ear out include either a small metal fixation plate as used here or a cadaveric rib graft. (I have yet to see a patient that opts for a rib graft harvest) No matter what is used it must be rigid enough that it holds the eat out securely when edged in behind it.
The effect of the otoplasty reversal procedure was immediate with the helical rim profile being now seen above that of the anti helical rim. Options to stabilize or hold the ear out include either a small metal fixation plate as used here or a cadaveric rib graft. (I have yet to see a patient that opts for a rib graft harvest) No matter what is used it must be rigid enough that it holds the eat out securely when edged in behind it.
Case Highlights:
1) The most common area that is overcorrected in a traditional otoplasty is the middle third of the ear helical rim which is seen by having the outer helical rim beneath the profile of the anithelical rim.
2) An otoplasty reversal in most cases is really a partial reversal or the treatment of one area of the ear that is overcorrected.
3) A delayed otoplasty reversal is based on cartilage release and the placement of an interpositional graft or device that will hold the ear out until it has fully healed.
Dr. Barry Eppley
Indianapolis, Indiana