

Background: The normally quiescent scrotum that draws little attention can become a major focus when it dramatically enlarges. There are a variety of causes for scrotal enlargement including injury, genital and pubic mound surgery, inguinal hernias, testicular torsion, varicoele, orchitis, hydrocoele and epididymitis to name the most common. In almost of of these causes once the source is properly treated and healing has occurred the scrotum will shrink back to normal. Acute scrotal edema almost always completely resolves.
Chronic scrotal edema/enlargement occurs from different sources. One of the common for refractory scrotal enlargement is lymphedema. If partial blockage occurs of the draining lymphatics or veins, the scrotum will remain edematous. There is no compression method to conservatively treat chronic scrotal lymphedema and make the scrotum smaller. Trying such compression may actually worsen the problem and may hinder the already limited blood supply to the scrotum. Further obstructing the venous outflow can increase the swelling. In addition the thin scrotal skin is not very tolerant of compression besides the obvious difficulty. Chronic scrotal enlargement can only be reduced by surgery.
Case Study: This 32 year-old male presented with chronic scrotal enlargement, being roughly 2X to 3X its normal size. He had a history of some form of autoimmune skin infection of the groin, believed to be a form of psoriasis. It eventually become improved through the use Humira and daily low-dose antibiotics. While not 100% cured, it was 98% improved. This skin condition left him with a chronically enlarged scrotum with thickened skin and diffuse subcutaneous tissue thickening. Besides its appearance, it gave him difficulty with wearing clothes and chaffing of the groin and scrotal skin.
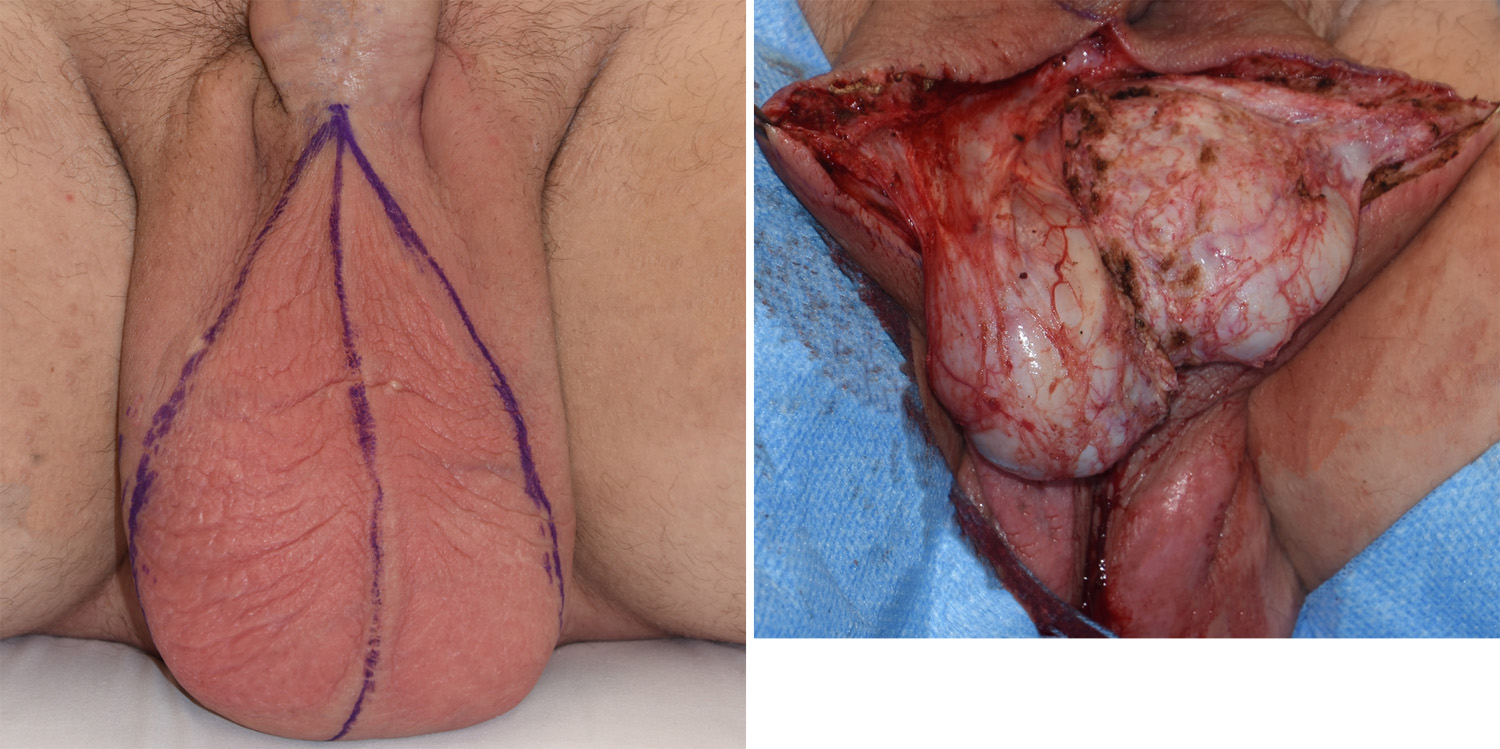
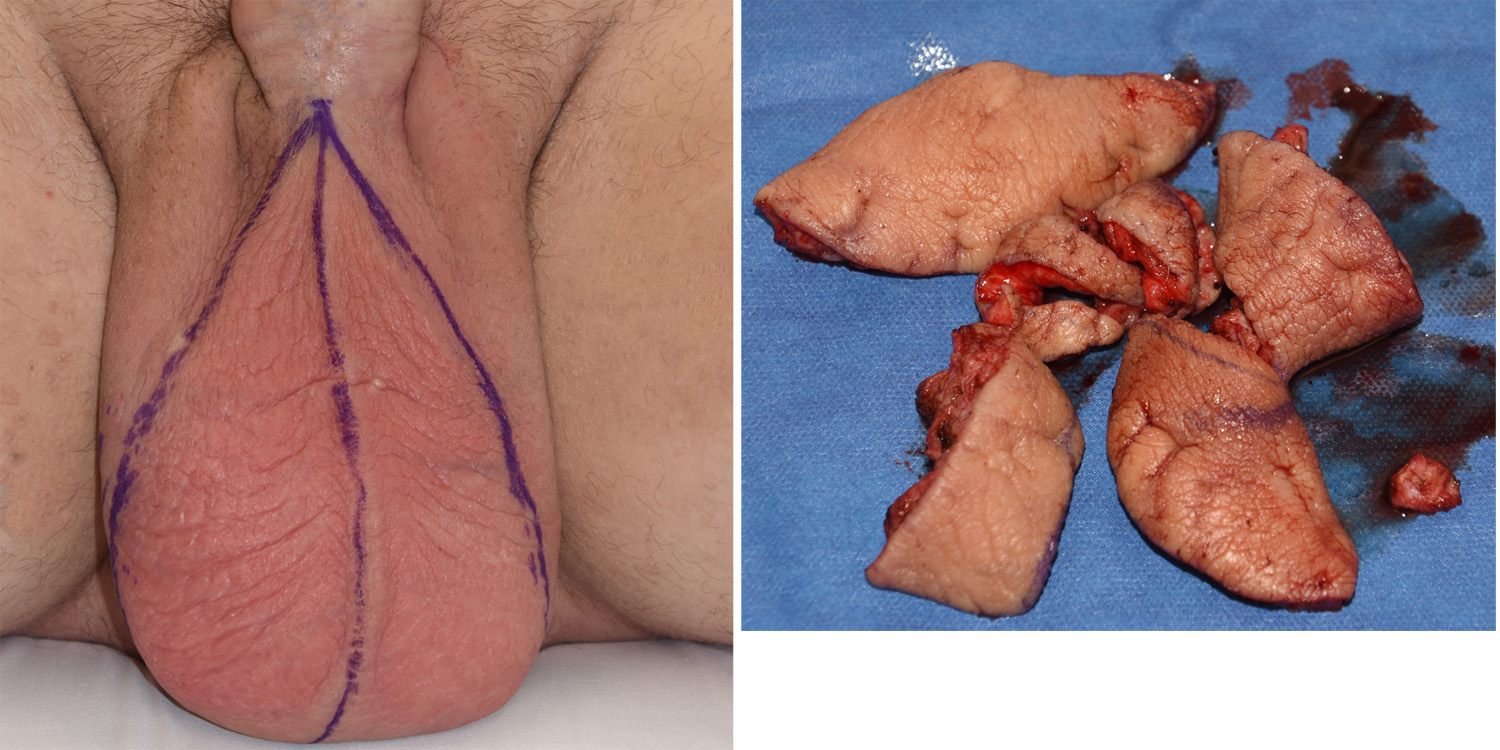
 Under general anesthesia and in a frog-legged position, a large elliptical excisional pattern was marked out vertically using the midline raphe as the center. The widest area of excision was 14 cms. The thickened skin and the watery expanded superficial fascial tissue were excised. The testicules and the enveloping tunica vaginalis lining were dissected out and preserved. Closure was done by covering the testicles with the remaining scrotal skin with a midline approximation.
Under general anesthesia and in a frog-legged position, a large elliptical excisional pattern was marked out vertically using the midline raphe as the center. The widest area of excision was 14 cms. The thickened skin and the watery expanded superficial fascial tissue were excised. The testicules and the enveloping tunica vaginalis lining were dissected out and preserved. Closure was done by covering the testicles with the remaining scrotal skin with a midline approximation.
A chronically enlarged scrotum can be effectively reduced by wide excision of the redundant tissues. The scar line should be placed along the naturally occurring midline raphe where a good scar outcome would be expected.
Highlights:
1) Permanent scrotal enlargement can occur from chronic skin infections that results in enlarged and abnormal skin
2) Scrotal reduction involves an elliptical excision of skin and fascia centered along the vertical midline raphe.
3) Scrotal reduction preserves the testicles and their surrounding sac.
Dr. Barry Eppley
Indianapolis, Indiana