

Background: Custom skull implants provide a new method for changing the shape of the head through their ability to add volume in a controlled preoperatively designed fashion. By definition this makes the scalp tighter. That is certainly true initially although some scalp relaxation undoubtably occurs later. This is well known to me as some skull implant patients go on after to have their implant changed to a bigger one which would only be possible of there was more scalp to stretch.
Browlift surgery can be done using several techniques. The most commonly used method, the endoscopic browlift, achieves its effect by a galeal shift or scalp translocation. The brows are lifted because the entire scalp shifts backward raising the eyebrows in the process. Excisional browlifts work by removing either forehead (hairline browlift) or scalp tissue (coronal browlift) to achieve a superior movement of the brow tissues.
An interesting question is can a browlift be done in a patient who has an indwelling skull implant. With the scalp expansion by an implant it would seem unlikely that an endoscopic brow lift can be effective because of the need for a significant galeal shift backwards. But a direct excisions approach should be unaffected as it does not rely on scalp elasticity.
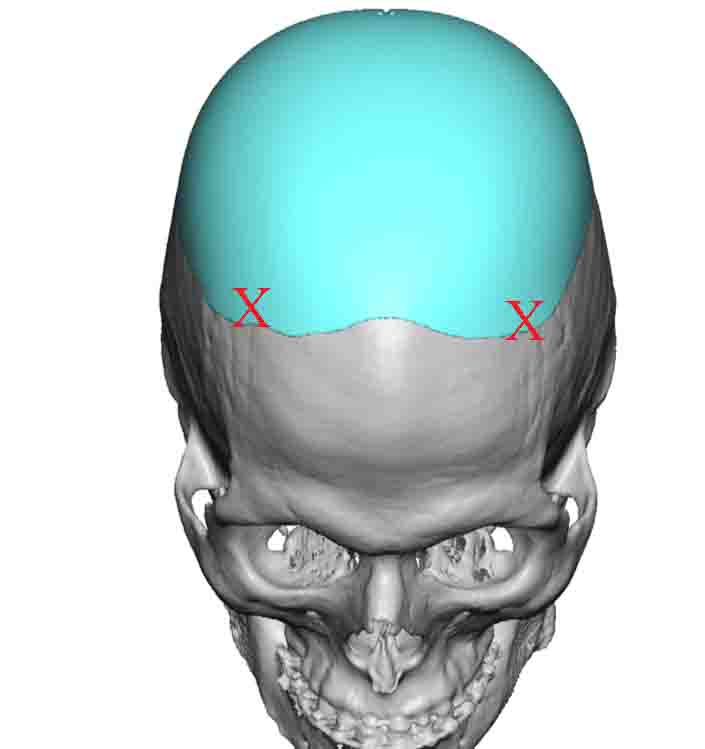
Case Study: This male wanted a temporal browlift to raise the outer half of his brows so that he did not have a horizontal brow shape. He had a history of a prior custom skull implant that stretched from his frontal hairline back to the mid-occipital region. It was decided that a hairline approach would be used in the temporal area to do a direct type of browlift.
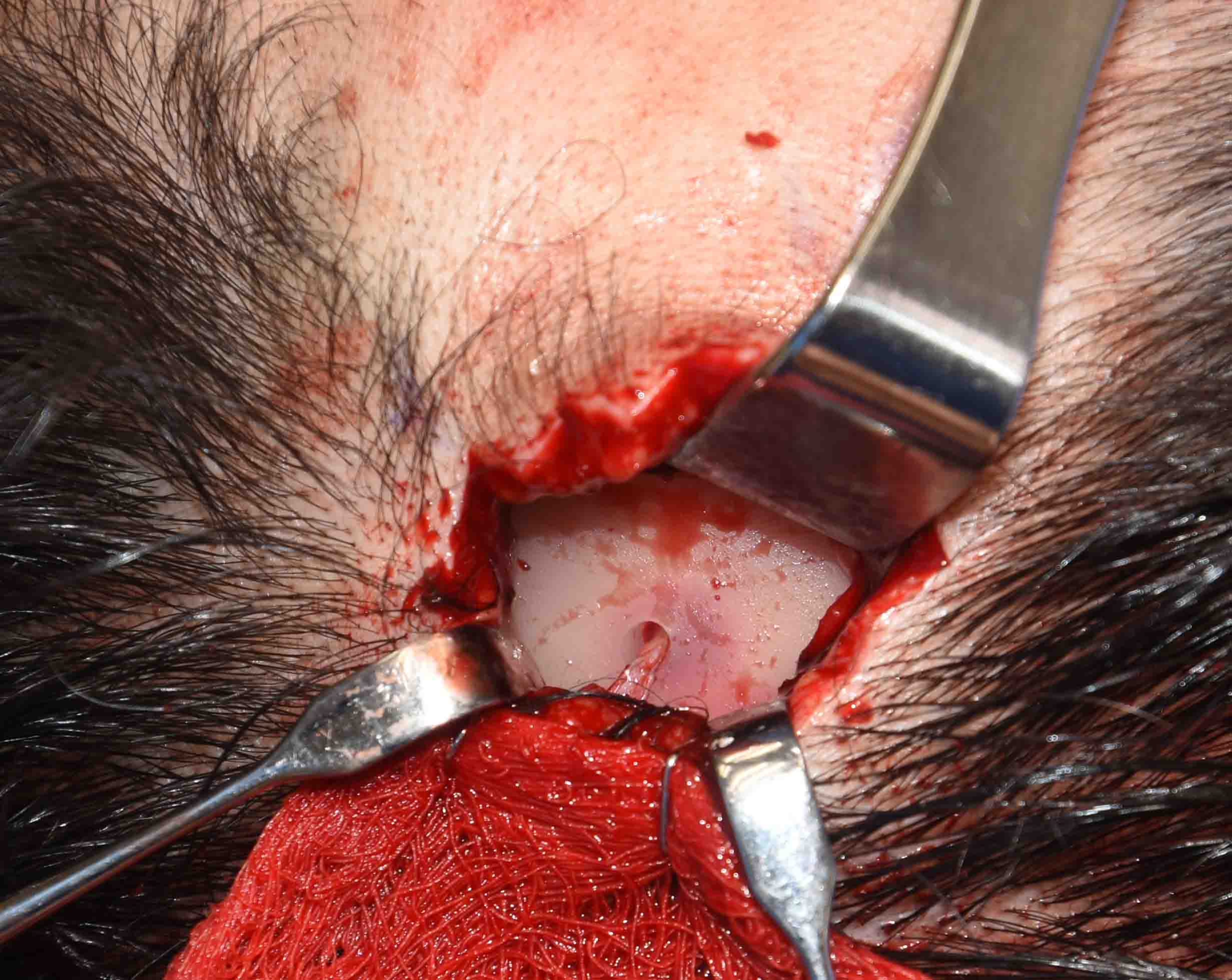
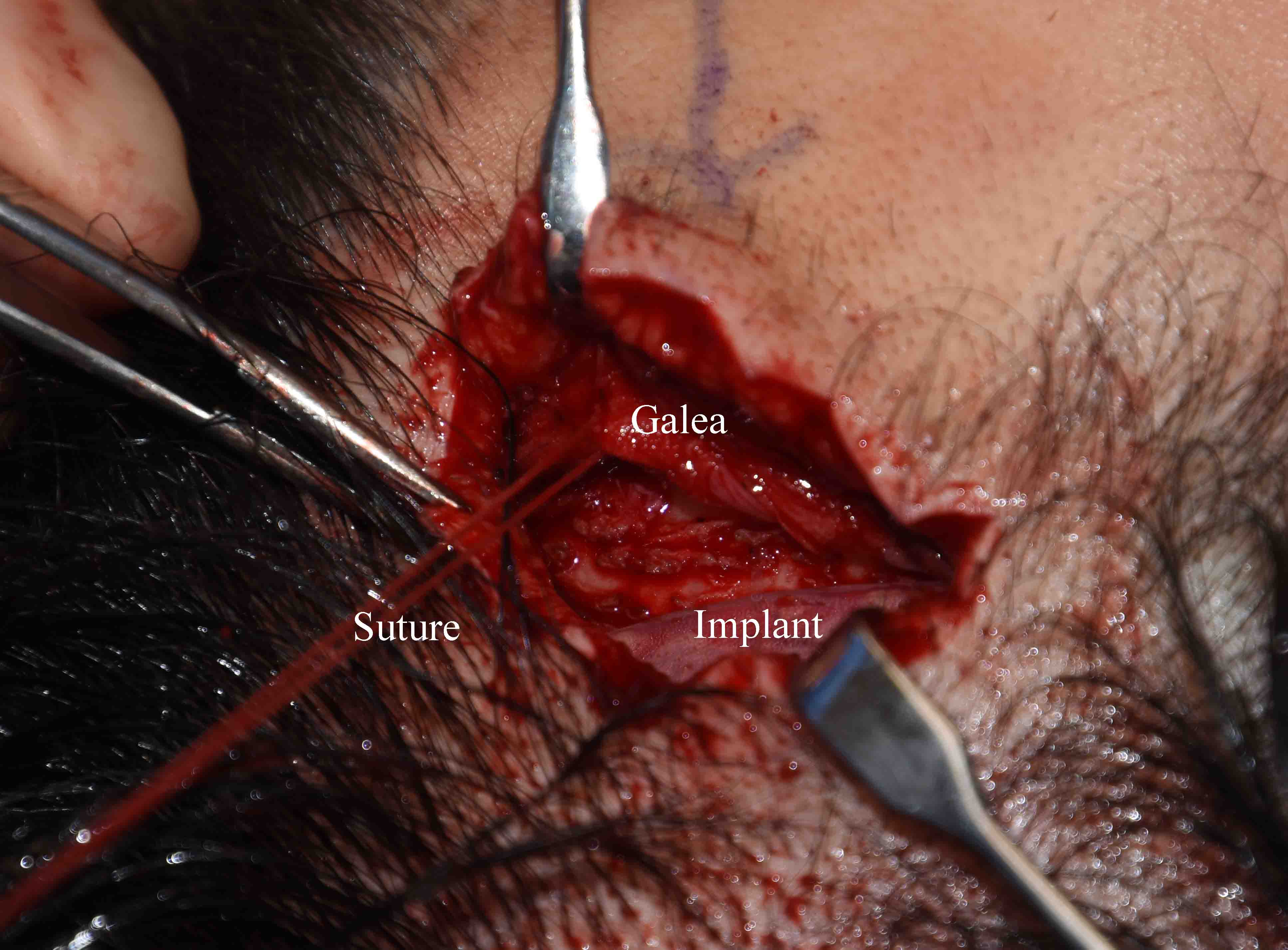
 Under general anesthesia, an irregular hairline incision was done along the temporal area in a line directly along the vector needed for the browlift. In dissecting down to the bone the edge of the skull implant was encountered. The soft tissue ingrowth could be seen into the holes in the implant. Subperiosteal dissection was done down to the lateral orbital rim and the periosteum was released. The front edge of the skull implant served as the fixation points for the galeal sutures to support the lifted temporal brows from the subperiosteal release.
Under general anesthesia, an irregular hairline incision was done along the temporal area in a line directly along the vector needed for the browlift. In dissecting down to the bone the edge of the skull implant was encountered. The soft tissue ingrowth could be seen into the holes in the implant. Subperiosteal dissection was done down to the lateral orbital rim and the periosteum was released. The front edge of the skull implant served as the fixation points for the galeal sutures to support the lifted temporal brows from the subperiosteal release.
Case Highlights:
1) Browlifting in a patient with an indwelling skull implant poses new territory in whether it can be effectively done.
2) In the direct hairline approach to a temporal browlift the implant can serve as points of soft tissue fixation.
3) The skull implant can be seen to have tissue ingrowth through its perfusion holes.
Dr. Barry Eppley
Indianapolis, Indiana