

Background: At its most simplistic level, aesthetic skull augmentation uses an implant to push off the outer bony cortex to create an overlying soft tissue expansion the scalp. Like every form of aesthetic face and body augmentation the ability of the soft tissues to stretch and be displaced outward is ultimately what creates the change in the external contour appearance.
Unlike most other soft tissue areas of the face or body, the scalp of the skull is unique. Because it is covering a spherical surface, the scalp has a certain degree of natural tightness. No one would appreciate or look very good if the scalp was loose and hung down onto the face. While some scalps are more stretchy (elastic) than others, there is a defined limit as to how much it can stretch to accommodate an implant underneath it. Since a skull implant is curved to match the shape of the skull bone and often covers a large surface area, it exerts a fair amount of pressure on an already tight overlying scalp.
In consideration of the ability of the scalp to accommodate an underlying implant and have a competent scalp closure, larger skull augmentation will require a first stage scalp expansion process. But unlike what is done in scalp reconstruction where the such expansions are considerable to replace missing portions of the scalp, expansion for skull augmentations are more modest in size and entail a much shorter time between its placement and when the skull implant can be done.
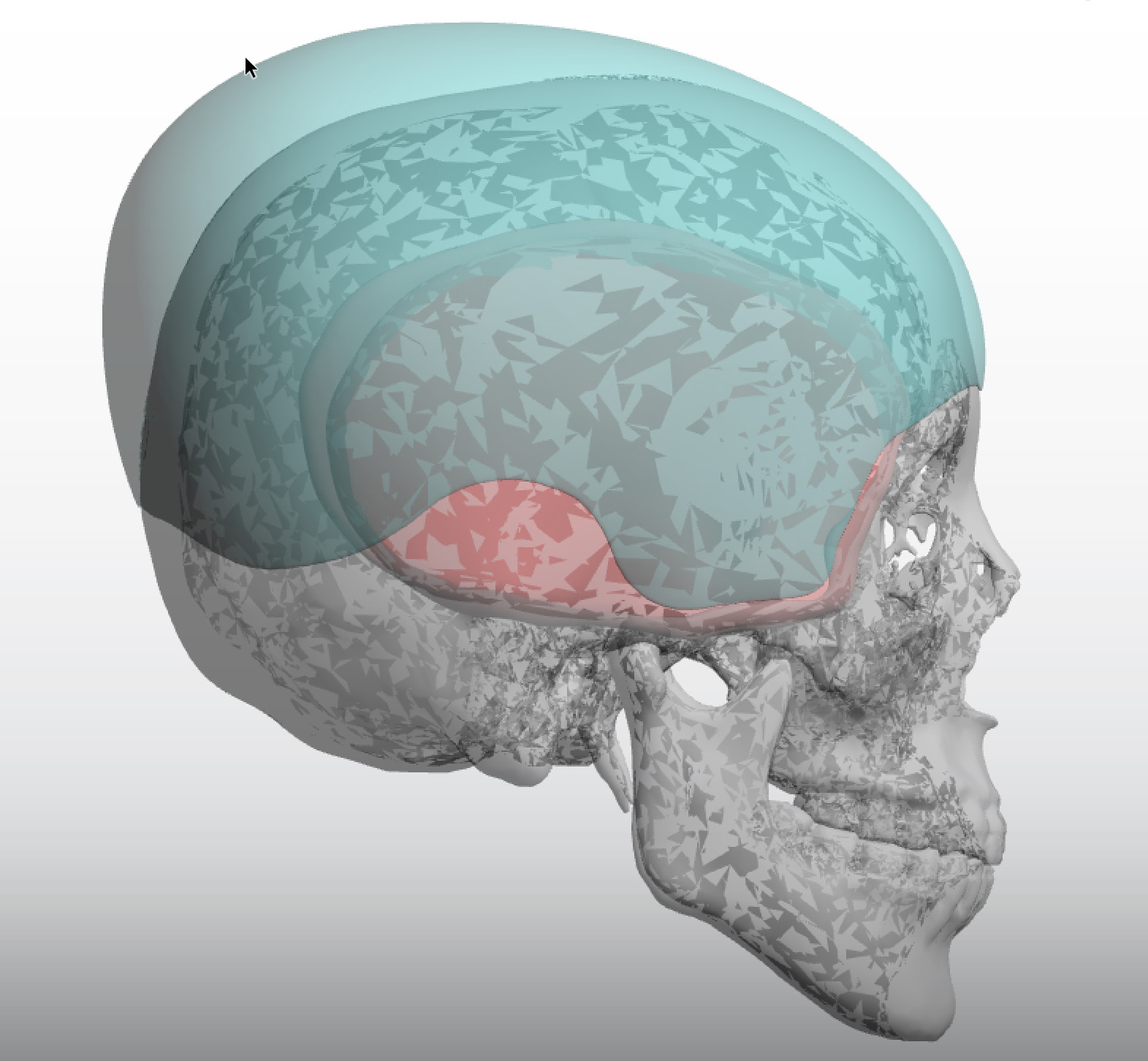
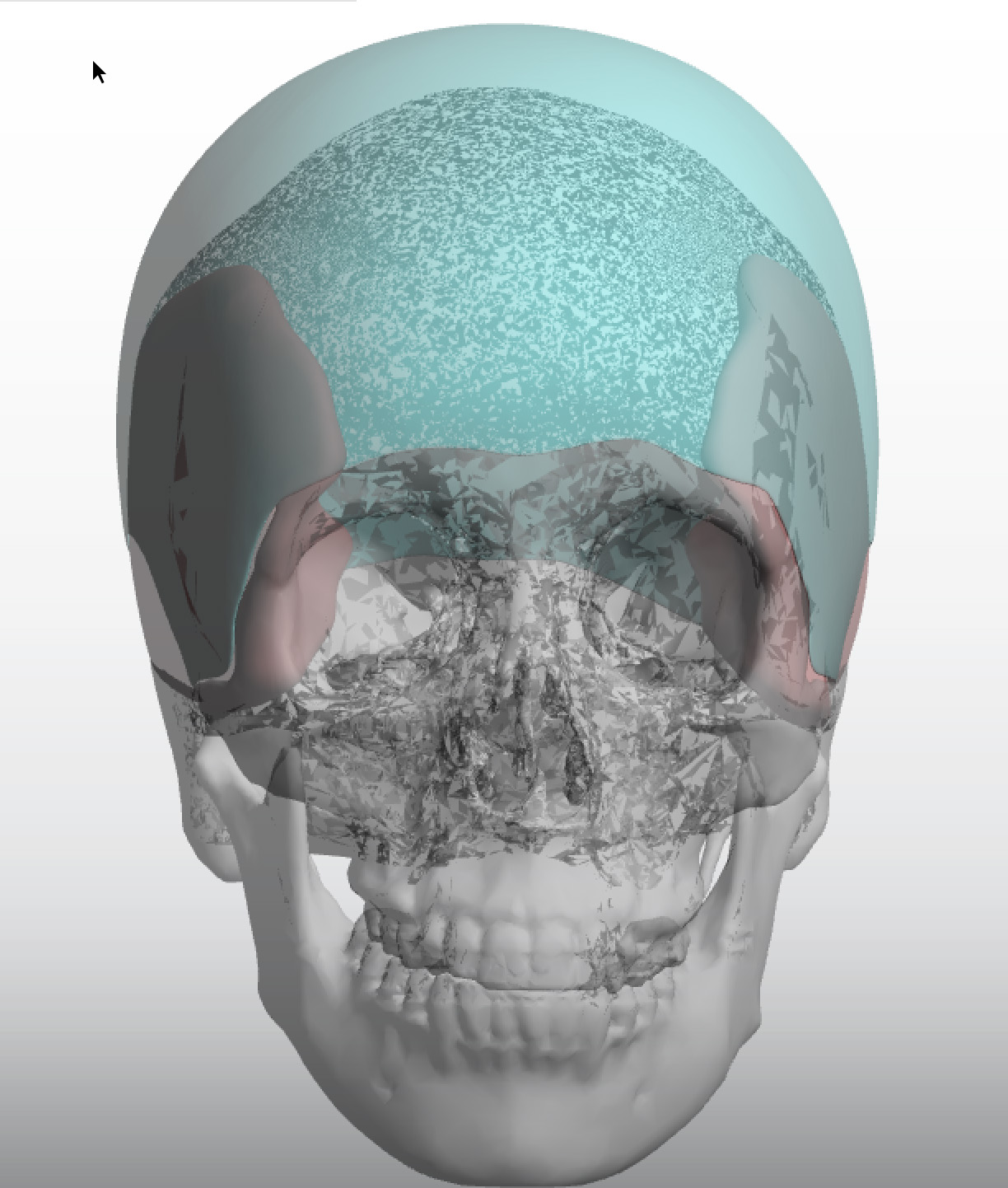 Case Study: This young female desired a considerable skull augmentation from the forehead-temporal area the whole way back to the bottom of the occiput. Given that the preoperative implant volume was estimated at close to 300ccs, a first stage scalp expansion was needed.
Case Study: This young female desired a considerable skull augmentation from the forehead-temporal area the whole way back to the bottom of the occiput. Given that the preoperative implant volume was estimated at close to 300ccs, a first stage scalp expansion was needed.
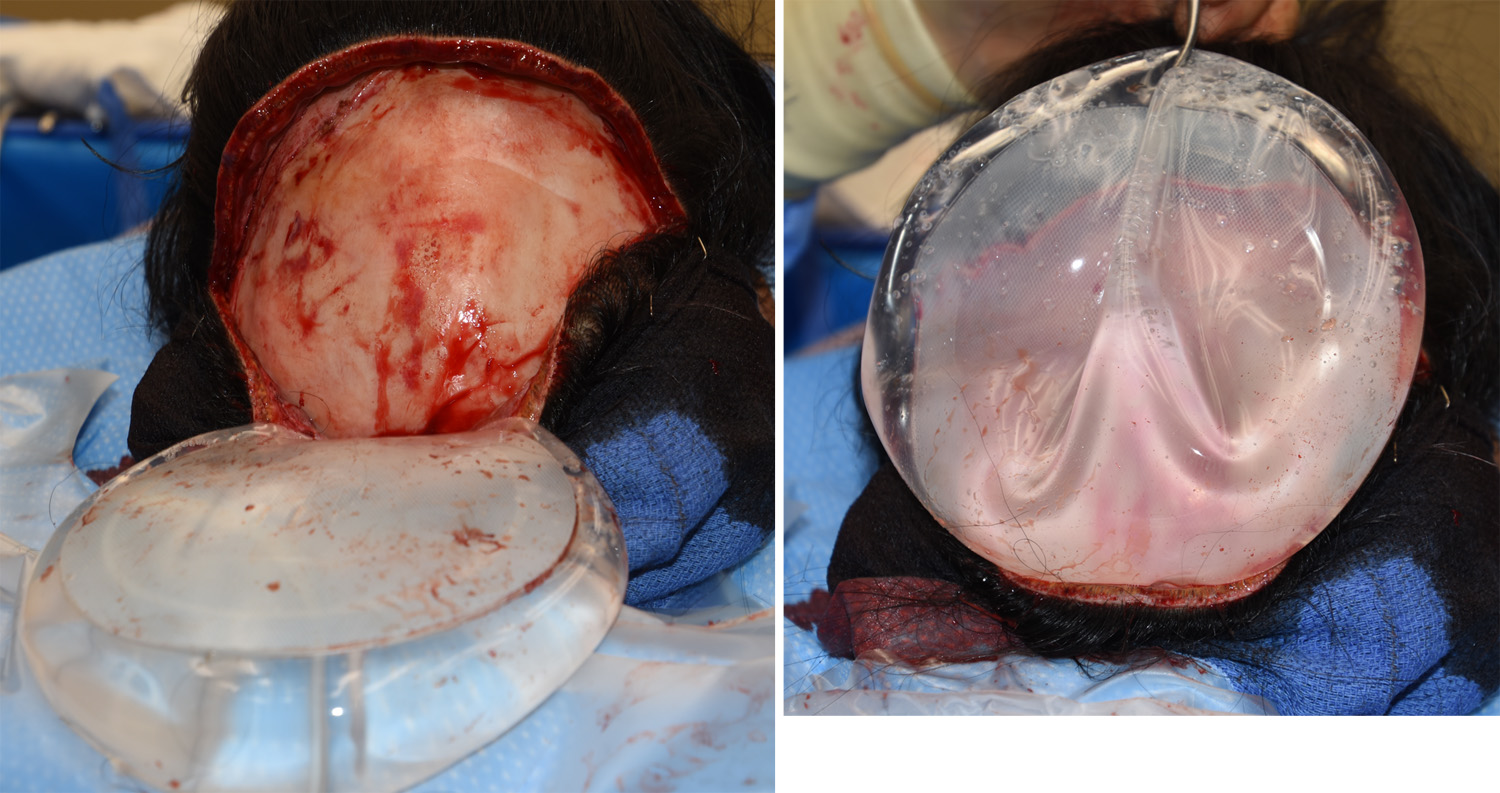 In the first stage a circular scalp expander was placed that was capable of up to 550ccs of instilled volume. However the scalp expansion goal was closer to 300ccs to match that of the designed implant volume. When removed six weeks later, the expander shows that it was partially filled (55% of its potential volume) as would be expected with only a partial fill.
In the first stage a circular scalp expander was placed that was capable of up to 550ccs of instilled volume. However the scalp expansion goal was closer to 300ccs to match that of the designed implant volume. When removed six weeks later, the expander shows that it was partially filled (55% of its potential volume) as would be expected with only a partial fill.
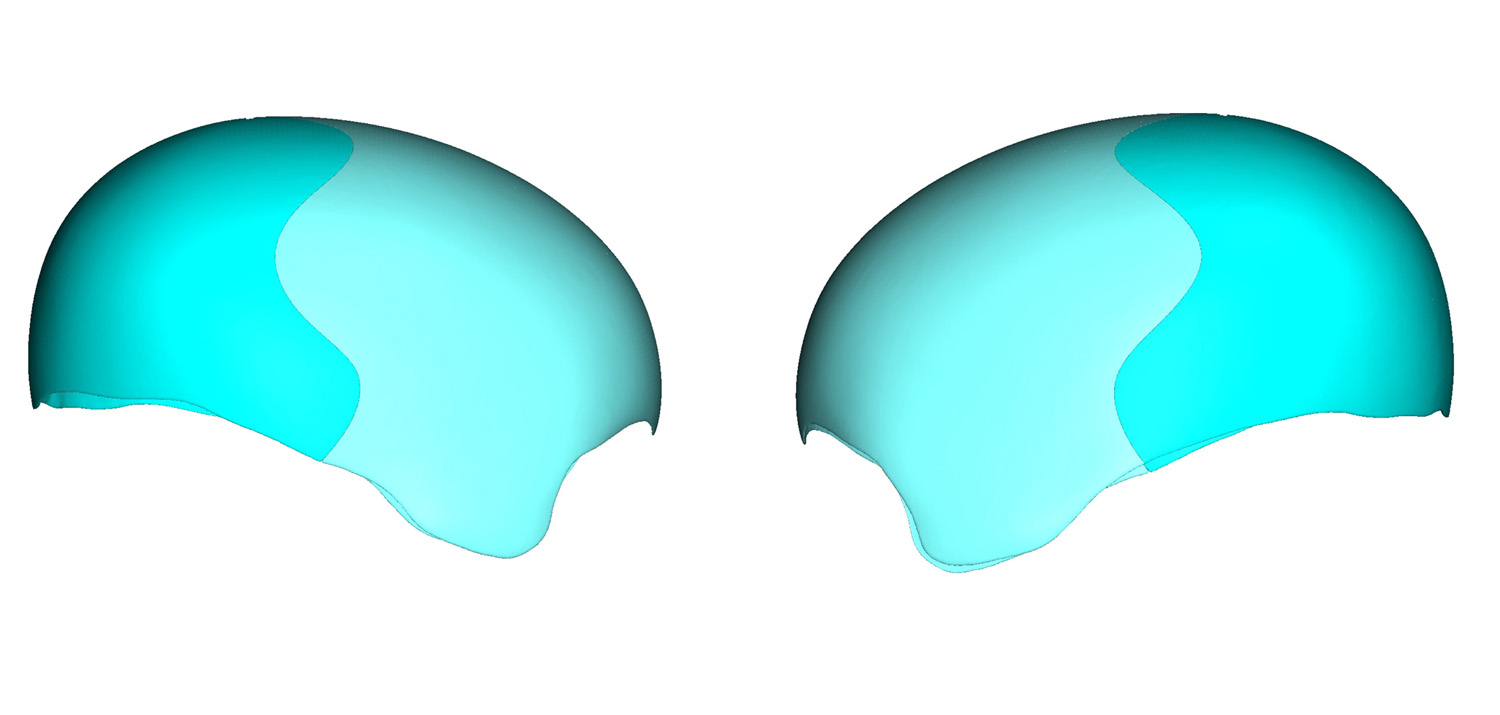
 The large skull implant was placed as designed, in two pieces, which are reunited once in place. The ‘reunion’ is first done with large sutures for alignment and then long fixation screws are staggered along the implant edges.
The large skull implant was placed as designed, in two pieces, which are reunited once in place. The ‘reunion’ is first done with large sutures for alignment and then long fixation screws are staggered along the implant edges.
What is not obvious in large skull augmentation cases is that a scalp expansion allows for a smaller scalp incision as well as allows for a larger skull implant. While a full coronal scalp incision from ear to ear will allow for some additional scalp mobility (although not enough to avoid the need for a scalp expander), the size of the scalp incision can be lessened through the preoperative scalp expansion.
Case Highlights:
1) Skull augmentation is unique in that the amount of soft tissue coverage must be strongly considered in the implant design.
2) In larger skull augmentation a first stage scalp expansion must be done to ensure competent scalp closure.
3) Scalp expansions for aesthetic skull augmentation are only done to about the size of the skull augmentation needed.
Dr. Barry Eppley
Indianapolis, Indiana