

Background: Skull defects come in a wide variety of shape, sizes and thicknesses. Correcting them can also be done using a variety of cranioplasty materials. The choice of cranioplasty material depends on a variety of factors including size of the defect, whether it is partial or full-thickness, and the desired location and length of the incision. The smaller the skull defect the more restrictive the cranioplasty options become.
The skull is prone to small contour defects caused by in utero and postnatal positioning, early trauma, and aberrant development. While many people have a perfectly smooth skull surface throughout there are just as many that do not. Many small skull defects are obscured by hair and are aesthetically irrelevant. But in an era where many men now shave their heads or have very short haircuts, the small skull contour defect may become revealed. Or at the least the person may perceive that it is visible.
Small skull defects can be treated by a semi-injection approach (small incision with introduction by an open barreled small syringe) using either different bone cement and substitute materials. (e.g., hydrocyapatite or HTR granules) While they can be effective they are prone to irregularities and are difficult to recontour secondarily.
Case Study: This 30 year old male had a skull indentation at the left temporo-parietal region that measured 5 x 3 cm. It had an indentation depth of 6 to 7mms in the center that feathered upward into the surrounding skull bone. It was very palpable and it had been present as long as the patient could remember.
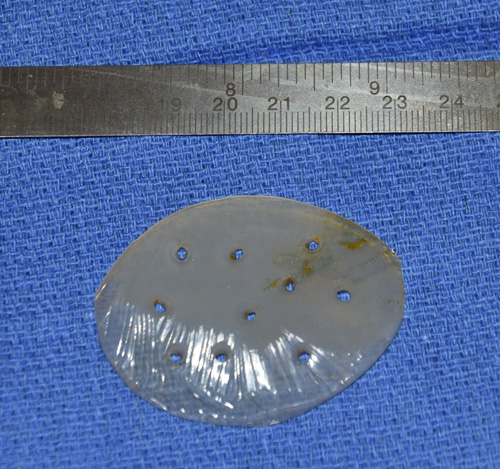
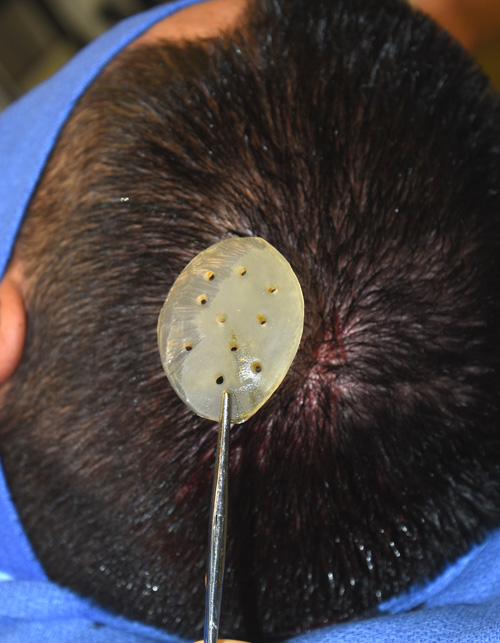 Under general anesthesia a 3 cm vertical scalp incision was made at the back end of the skull defect. Subperiosteal undermining in a circumferential manner around the defect edges extending it 1 cm beyond its borders. A silicone implant was hand carved with a scalpel from a preformed posterior temporal implant design. The thickest part was in the middle and the entire perimeter of the implant was trimmed to a feather edge. Perfusion holes of 3mms diameter were placed and the implant inserted and secured with a single 1.5mm screw at its posterior edge. The scalp was closed with dissolveable sutures and n dressing was used.
Under general anesthesia a 3 cm vertical scalp incision was made at the back end of the skull defect. Subperiosteal undermining in a circumferential manner around the defect edges extending it 1 cm beyond its borders. A silicone implant was hand carved with a scalpel from a preformed posterior temporal implant design. The thickest part was in the middle and the entire perimeter of the implant was trimmed to a feather edge. Perfusion holes of 3mms diameter were placed and the implant inserted and secured with a single 1.5mm screw at its posterior edge. The scalp was closed with dissolveable sutures and n dressing was used.
Skull implants to augment smaller contour defects can be done using silicone implant materials. Such material compositions are easy to shape and insert through a very discrete incision.
Highlights:
1) Small defects of the skull can be corrected by small silicone implants.
2) In very small skull defects, hand carved silicone skull implant can be made during surgery.
3) The incision used to place a small skull implant is usually no more than an inch or so.
Dr. Barry Eppley
Indianapolis, Indiana