

Background: The shape of the forehead is very gender specific and these differences are well known. The male forehead has prominent brow ridges, a brow bone break and a forehead that has a slight backward slope. The female forehead has no visible brow ridging or break and a more convex shape as it extends upward into the frontal hairline. These forehead shape differences are driven largely by the influence of testosterone on the development of the frontal sinuses and the frontal bone.
 In facial feminization surgery (FFS), forehead recontouring is an important one-third of the facial changes needed. This is usually perceived as ‘burring of the brow bone’ but this is an overly simplistic understanding of how to reshape the entire superior orbital rim. Because of the thinness of the outer cortex of the brow bone with a large underlying frontal sinus air space, simple burring of the frontal bone can only make a limited change. Most brow bone reductions of any significance require an osteoplastic bone flap technique in which the entire outer cortex is removed, reshaped and replaced.
In facial feminization surgery (FFS), forehead recontouring is an important one-third of the facial changes needed. This is usually perceived as ‘burring of the brow bone’ but this is an overly simplistic understanding of how to reshape the entire superior orbital rim. Because of the thinness of the outer cortex of the brow bone with a large underlying frontal sinus air space, simple burring of the frontal bone can only make a limited change. Most brow bone reductions of any significance require an osteoplastic bone flap technique in which the entire outer cortex is removed, reshaped and replaced.
But the brow bone reduction is often not enough to get a definitive gender change in the FFS patient. As part of the brow recontouring, the lateral or tail of the brow bone must be reduced to allow a more upward sweep to the tail of the eyebrow. In some cases, the orbital rim reduction may need to be carried around to the side to help with greater orbital exposure. (opening of the eye) Also, the frontal hairline may benefit from being advanced or lowered. If access to the brow bone reduction is done through a hairline or pretrichial approach, then vertical forehead reduction/hairline repositioning can be done at the same time as the brow bone reduction.
Case Study: This 35 year-old patient was undergoing a variety of facial feminization surgeries from the forehead down to the adam’s apple. The concerns on the forehead was that the brow bones were too strong but the upper forehead was adequately shaped/projected. The hairline was also in good place (not too high) with reasonable hair density.
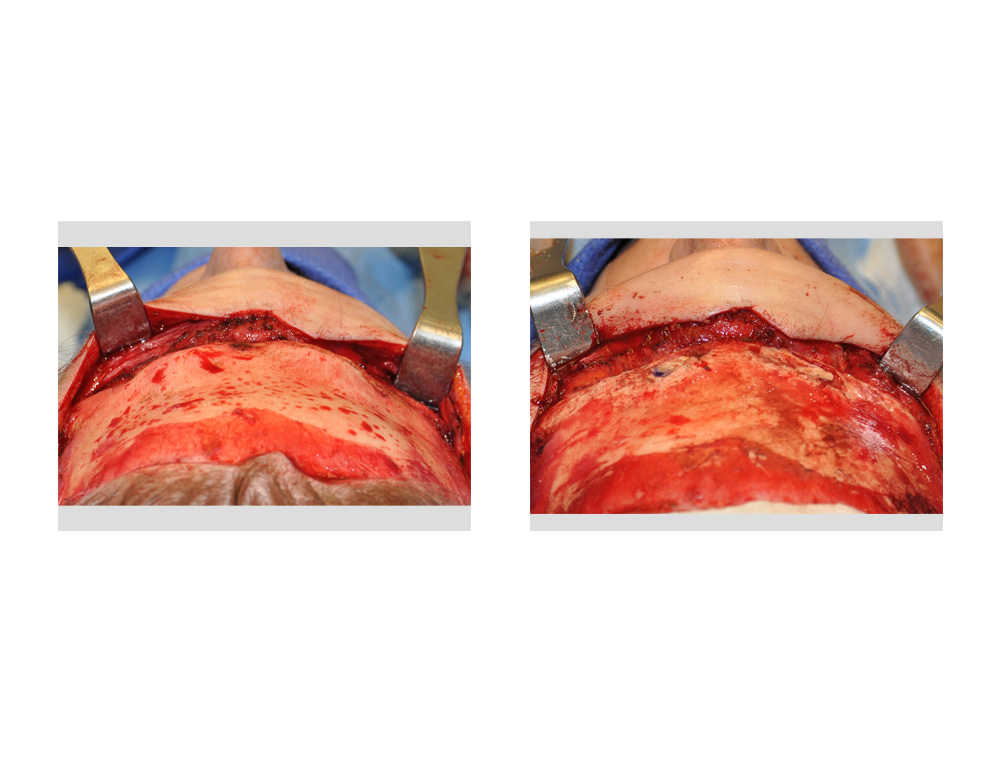
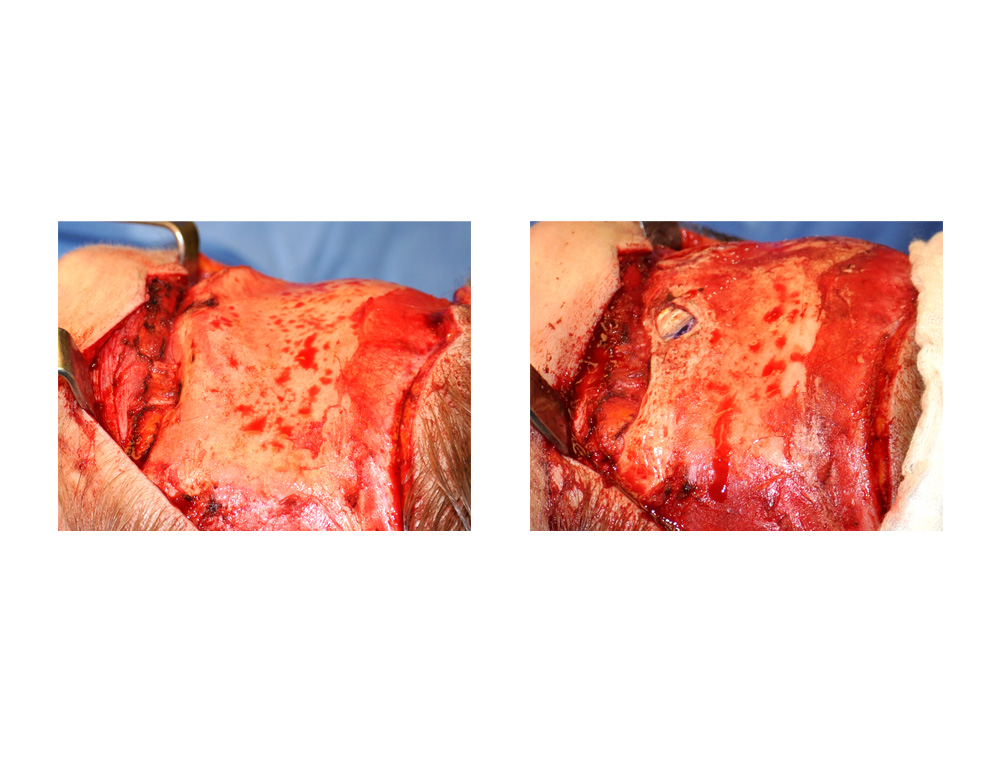 Under general anesthesia, a pretrichial or frontal hairline incision was made in an irregular fashion paralleling the direction of the hair shafts. The forehead flap was turned down and the brow bones exposed, protecting the supraorbital nerves. A reciprocating saw was used to take off the outer brow bones at the levels of the surrounding forehead. The two pieces were reshaped and put back with resorbable sutures. The tail of the brow bones were the frontal sinus cavities did not exist was burred done to reduce its prominence. The forehead flap was put back in a two layer closure with small sutures for the skin.
Under general anesthesia, a pretrichial or frontal hairline incision was made in an irregular fashion paralleling the direction of the hair shafts. The forehead flap was turned down and the brow bones exposed, protecting the supraorbital nerves. A reciprocating saw was used to take off the outer brow bones at the levels of the surrounding forehead. The two pieces were reshaped and put back with resorbable sutures. The tail of the brow bones were the frontal sinus cavities did not exist was burred done to reduce its prominence. The forehead flap was put back in a two layer closure with small sutures for the skin.

 Brow bone reduction is usually more than just simple burring, particularly with the goal of changing a prominent masculine brow shape to a flatter more feminine one. The osteoplastic bone flap technique is needed with the potential for additional procedures of lateral orbital rim contouring, forehead augmentation and hairline advancement done at the same time.
Brow bone reduction is usually more than just simple burring, particularly with the goal of changing a prominent masculine brow shape to a flatter more feminine one. The osteoplastic bone flap technique is needed with the potential for additional procedures of lateral orbital rim contouring, forehead augmentation and hairline advancement done at the same time.
Case Highlights:
1) Brow reduction is an important part of many facial feminization surgeries.
2) Brow reduction can be done by burring but usually needs a more aggressive approach with an osteoplastic bone flap to create a more feminine brow shape.
3) Many FFS brow bone reductions can be done through a hairline or pretrichial incision which allows for a simultaneous hairline advancement if desired.
Dr. Barry Eppley
Indianapolis, Indiana