

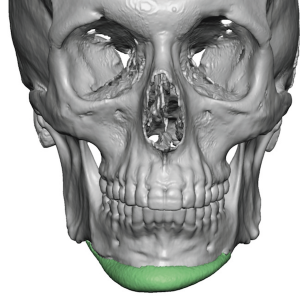
 The chin implant is viewed as a low risk facial augmentation procedure and it is certainly the most commonly done. In theory it is the easiest of all facial implants to perform as the incisional access is very close to the implantation site (whether it is intraoral or submental), it is a single implant over a solitary projecting bone area and there is little neurovascular anatomy in the path of the dissection. In today’s anatomic or extended chin implants getting the implant centered at the midline of the chin bone is but one surgical objective. Ensuring that the wings of the implant are laying completely flat along the lower rim of the chin is another element of ideal positioning where the implant can exert its best aesthetic effect.
The chin implant is viewed as a low risk facial augmentation procedure and it is certainly the most commonly done. In theory it is the easiest of all facial implants to perform as the incisional access is very close to the implantation site (whether it is intraoral or submental), it is a single implant over a solitary projecting bone area and there is little neurovascular anatomy in the path of the dissection. In today’s anatomic or extended chin implants getting the implant centered at the midline of the chin bone is but one surgical objective. Ensuring that the wings of the implant are laying completely flat along the lower rim of the chin is another element of ideal positioning where the implant can exert its best aesthetic effect.
 Having said that, malposition of the chin implant is not uncommon despite the seemingly simplicity of the operation. Having seen thousands of 3D CT scans chin implants can appear in all sorts of adverse placements around the chin bone. This may seem incredulous but it is important to remember that it is not as easy as putting an implant on skeletal model. Access is through a very limited incision compared to the length of the implant for placement and absolute visibility of all aspects of the implant’s position on the bone is not possible. Perhaps surprisingly to patients is that much facial implant placements are partially ‘blind’ and the chin implant is no exception.
Having said that, malposition of the chin implant is not uncommon despite the seemingly simplicity of the operation. Having seen thousands of 3D CT scans chin implants can appear in all sorts of adverse placements around the chin bone. This may seem incredulous but it is important to remember that it is not as easy as putting an implant on skeletal model. Access is through a very limited incision compared to the length of the implant for placement and absolute visibility of all aspects of the implant’s position on the bone is not possible. Perhaps surprisingly to patients is that much facial implant placements are partially ‘blind’ and the chin implant is no exception.
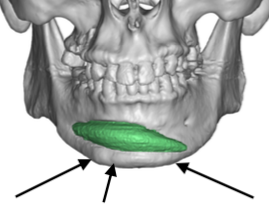
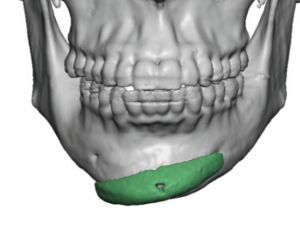 One of the most common types of chin implant malpositions is were one or both of the wings are angulated upward, significantly away from their ideal line of placement. Or the entire chin implant is very highly positioned on the bone.
One of the most common types of chin implant malpositions is were one or both of the wings are angulated upward, significantly away from their ideal line of placement. Or the entire chin implant is very highly positioned on the bone.
 This is due to failure of release of the numerous osteocutaneous ligaments along the chin. These ligamentous attachments as seen in 3D CT scans as bumps on the bone.These very strong attachments provide resistance to the subperiosteal elevation along the inferolateral chin bone and it is very easy to just slide above them where the dissection is much easier. Lack of ligament release stems from failure to recognize that these ligaments are even present and their relevance to good chin implant placement. Unfortunately it is an anatomic realization of which many surgeons are not aware.
This is due to failure of release of the numerous osteocutaneous ligaments along the chin. These ligamentous attachments as seen in 3D CT scans as bumps on the bone.These very strong attachments provide resistance to the subperiosteal elevation along the inferolateral chin bone and it is very easy to just slide above them where the dissection is much easier. Lack of ligament release stems from failure to recognize that these ligaments are even present and their relevance to good chin implant placement. Unfortunately it is an anatomic realization of which many surgeons are not aware.
Besides aesthetic issues (asymmetry, lack of adequate projection) that occur with this superior displacement of part or all of the chin implant, this forces its wings up against, into or even above the mental nerve at its exit from the bone. This is the most common cause of persistent numbness or pain after chin implant surgery.
An integral part of any chin implant placement is adequate soft tissue release which defines the subperiosteal pocket. Part of this soft tissue release is that of the osteocutaneous ligaments. One release can cause the implant to be sitting too low so this is also part of the dissection in which to be vigilant. But far more commonly is their under release and high riding implants on the bone.
Dr. Barry Eppley
Indianapolis, Indiana