

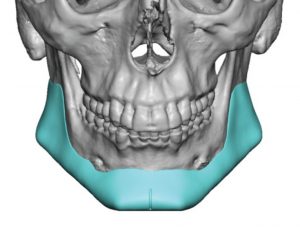
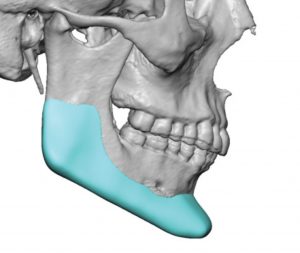
 Custom jawline implants provide the most effective method of augmentation of the lower third of the face. Their complete surface area coverage of the infer lateral jawline assured the significant shape and volumetric enhancement in a connected fashion. Of patients who present for such jawline augmentation about 40% have prior implants in place.
Custom jawline implants provide the most effective method of augmentation of the lower third of the face. Their complete surface area coverage of the infer lateral jawline assured the significant shape and volumetric enhancement in a connected fashion. Of patients who present for such jawline augmentation about 40% have prior implants in place.
Whether it is a standard chin implant, isolated standard jaw angle implants or combined standard chin and jaw angle implants, their presence is both a benefit and a liability. Their benefit is that knowing what lies wherein and what its aesthetic effects are allows for designing an implant replacement that can be better. Keeping what is good about the current implants (provided there is something) and adding to what it doesn’t do creates less guesswork about what the potential aesthetic effects of a new implant design could do.
 The liabilities of indwelling chin and jaw implants are numerous. Not all implant materials can be equally seen in 3D CT scans. Silicone, Gore-tex and PEEK/PEKK material compositions appear clearly while Medpor (porous polyethylene) does not. The tissue ingrowth that occurs with Medpor makes it ‘invisible’ in 3D scans. This poses a lack of information to aid in the new implant design. Sometimes the material will leave an imprint on the bone which can outline at least the location on the bone as to where the implant is.
The liabilities of indwelling chin and jaw implants are numerous. Not all implant materials can be equally seen in 3D CT scans. Silicone, Gore-tex and PEEK/PEKK material compositions appear clearly while Medpor (porous polyethylene) does not. The tissue ingrowth that occurs with Medpor makes it ‘invisible’ in 3D scans. This poses a lack of information to aid in the new implant design. Sometimes the material will leave an imprint on the bone which can outline at least the location on the bone as to where the implant is.
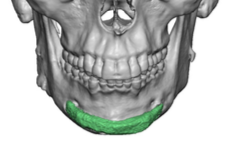
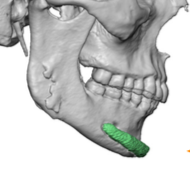 What is seen around all implant materials is imprinting onto the underlying bone of the implant’s footprint and any bony overgrowth. Bony overgrowth is a natural biologic reaction which indicates an effort at the bone to remodel. This occurs around the top and front edge of jaw angle implants and usually along the bottom and sides of chin implants. This bony overgrowth is going to have to be removed for the new implant to fit properly. Osteotomes usually work fine for this type of bone removal.
What is seen around all implant materials is imprinting onto the underlying bone of the implant’s footprint and any bony overgrowth. Bony overgrowth is a natural biologic reaction which indicates an effort at the bone to remodel. This occurs around the top and front edge of jaw angle implants and usually along the bottom and sides of chin implants. This bony overgrowth is going to have to be removed for the new implant to fit properly. Osteotomes usually work fine for this type of bone removal.
 While silicone and PEEK/PEKK materials do not get soft tissue attachments, Medpor and Goretex do. These tenacious attachments are major liabilities when they have to be removed. The trauma of removing these materials risk muscle, nerve and vessel injuries in addition to the time and tedious nature of doing so. They almost never can be removed in the manner in which they were placed. (single piece implant) The materials tear/fragment on removal. Having removed many of these materials there are cases where in the midst of it I question whether it can really be removed…but it has always been successfully done.
While silicone and PEEK/PEKK materials do not get soft tissue attachments, Medpor and Goretex do. These tenacious attachments are major liabilities when they have to be removed. The trauma of removing these materials risk muscle, nerve and vessel injuries in addition to the time and tedious nature of doing so. They almost never can be removed in the manner in which they were placed. (single piece implant) The materials tear/fragment on removal. Having removed many of these materials there are cases where in the midst of it I question whether it can really be removed…but it has always been successfully done.
 Between the need for capsulotomies, bone removal and existing implant removals, completing these necessary procedures often works to complete the extent of the subperiosteal dissection needed to place a wrap around jawline implant.
Between the need for capsulotomies, bone removal and existing implant removals, completing these necessary procedures often works to complete the extent of the subperiosteal dissection needed to place a wrap around jawline implant.
Dr. Barry Eppley
Indianapolis, Indiana