

 Aesthetic changes to the width of the shoulder can be done by a variety of surgical techniques. For shoulder width reduction only one surgical method exists…clavicular reduction osteotomies. Conversely shoulder augmentation can be done by three different methods which are performed at different shoulder locations. Deltoid muscle augmentation can be done by either injectable fat grafting or deltoid muscle implants. The length of the clavicles can also be expanded through osteotomies and bone grafting.
Aesthetic changes to the width of the shoulder can be done by a variety of surgical techniques. For shoulder width reduction only one surgical method exists…clavicular reduction osteotomies. Conversely shoulder augmentation can be done by three different methods which are performed at different shoulder locations. Deltoid muscle augmentation can be done by either injectable fat grafting or deltoid muscle implants. The length of the clavicles can also be expanded through osteotomies and bone grafting.
Each shoulder augmentation method has their own advantages and disadvantages. Any form of muscle augmentation is less invasive and has a quicker recovery although the overall shoulder widening effects may be more limited. Clavicle lengthening osteotomies are more invasive, have a much longer recovery but may also have more profound shoulder widening effects. There is, however, limited clinical experience with this type of aesthetic shoulder augmentation surgery.
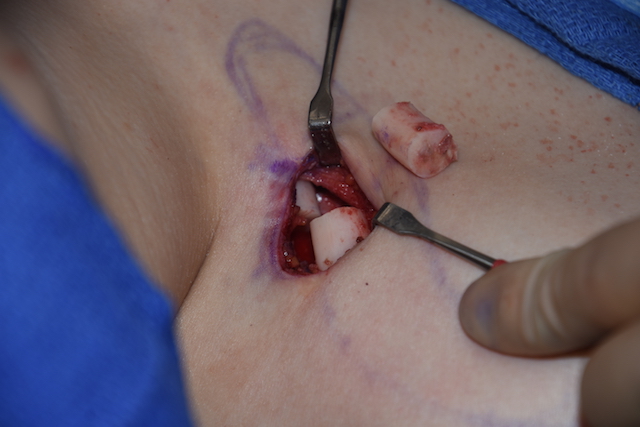
In the December 2016 issue of the journal Musculoskeletal Surgery a relevant article was published entitled ‘Congenital forward shoulder with clavicle hypoplasia: surgical lengthening by intercalary graft positioning and plate fixation.’ In this paper the authors describe an asymptomatic congenital condition of the shoulder associated with short clavicles and a more forward rolled shoulder position. Surgery was undertaken to improve aesthetic appearance. Three patients were treated by osteotomies and interpostional bone grafting with plate fixation. The surgical technique consisted of a long direct incision over the clayicle (12 to 14 cms in length), a mid shaft osteotomy, an interpositonal autologous iliac bone graft of about 1.5cms (which was wedged in and not secured to the plate) and 3.5cm plate fixation. (3 screws medially and two screws laterally)
All three patients healed without complications and were satisfied with their results. Followup was done up to two years after surgery. The plates and screws were eventually removed in all cases.
This small clinical series supports that the clavicles can be successfully lengthened with shoulder width increases with osteotomies and bone grafting. In order to transition the surgical techniques used in this paper as a more aesthetically acceptable procedure several modifications would need to be done. First the incision would need to be fat shorter in the 5 cms range. Second, like clavicular reduction the osteotomy would be done over the medial third of the clavicle where the incision could also be more favorably placed. Third, at least a 2.5cm length bone graft is needed that would be placed parallel to the shaft of the clavicle and would need to have a screw to attach it to the overlying plate.

 The one debate would be whether this clavicle bone graft should be autologous or allogeneic. Autologous graft is always best and the best donor site would be the fibula where the shape of the bone best matches the clavicle and more than adequate length can be harvested for both clavicle sides. (even though the orthopedic literature always uses an iliac graft) We know from extensive free fibular microsurgical reconstruction of the mandible that a long segments can be removed without adverse functional sequelae…but how many patients would want to go through this harvest site vs. an allogeneic (tissue bank) clavicle bone graft? The unknown issue is how long would it take for bone to grow across an allogeneic graft vs an autologous graft and would the risk of non-union be significantly higher with non-autologous grafts? The experience from treating clavicle fracture non-unions almost always uses autologous hip grafting but a clean osteotomy line over the medial third of the clavicle is a different clinical situation.
The one debate would be whether this clavicle bone graft should be autologous or allogeneic. Autologous graft is always best and the best donor site would be the fibula where the shape of the bone best matches the clavicle and more than adequate length can be harvested for both clavicle sides. (even though the orthopedic literature always uses an iliac graft) We know from extensive free fibular microsurgical reconstruction of the mandible that a long segments can be removed without adverse functional sequelae…but how many patients would want to go through this harvest site vs. an allogeneic (tissue bank) clavicle bone graft? The unknown issue is how long would it take for bone to grow across an allogeneic graft vs an autologous graft and would the risk of non-union be significantly higher with non-autologous grafts? The experience from treating clavicle fracture non-unions almost always uses autologous hip grafting but a clean osteotomy line over the medial third of the clavicle is a different clinical situation.
Dr. Barry Eppley
Indianapolis, Indiana