

Background
Male body types vary widely and are often associated with weight, but weight alone does not define body shape. For example, a lean individual may have thin subcutaneous tissues but good muscle mass, while someone of higher weight may carry more subcutaneous fat but possess limited muscle mass.
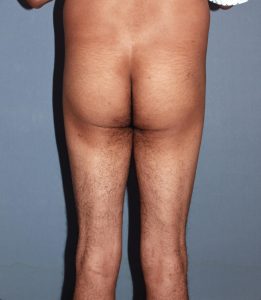
This distinction is especially relevant to the buttocks, where men with small buttocks and thin legs often present with both limited subcutaneous tissue and reduced muscle mass. Such patients are prone to a flat buttock and skinny-leg appearance.
In these cases, traditional buttock augmentation with fat injections (BBL) is not an option due to the lack of donor fat. Implants become the only viable solution. For thin patients, the intramuscular implant pocket is preferred. It reduces the risks of implant show, positional shifting, infection, and seroma formation. The tradeoff is that implant size is limited. Attempting to place larger implants above the muscle increases the likelihood of implant visibility, flipping, and migration—complications that outweigh the perceived benefits.
However, augmenting the buttocks alone in flat-buttock, skinny-leg males may result in disproportion, with the legs appearing too thin relative to the enhanced buttocks. This raises the question of whether thigh augmentation could restore balance. Although less common and not widely known, thigh augmentation with custom implants can be performed for regional leg enlargement.
Case Study
A male patient presented with a thin lower body lacking curves and desired combined buttock and thigh augmentation.

 Under general anesthesia and in the prone position, an intergluteal incision was made to expose the gluteus maximus muscle. The muscle was split, and an intramuscular pocket was created. Into this, 400cc solid, low-durometer buttock implants were placed. Multilayer closure was performed without drains.
Under general anesthesia and in the prone position, an intergluteal incision was made to expose the gluteus maximus muscle. The muscle was split, and an intramuscular pocket was created. Into this, 400cc solid, low-durometer buttock implants were placed. Multilayer closure was performed without drains.


 The patient was then positioned supine. A high anterolateral incision was made to expose the fascia of the biceps femoris and vastus lateralis muscles. A subfascial pocket was developed, and long thigh implants were inserted. Again, multilayer closure was performed without drains.
The patient was then positioned supine. A high anterolateral incision was made to expose the fascia of the biceps femoris and vastus lateralis muscles. A subfascial pocket was developed, and long thigh implants were inserted. Again, multilayer closure was performed without drains.


 At long-term follow-up, the patient showed significant improvement in body shape between the waist and knees. The thigh implants complemented the buttock implants, producing a more proportionate and aesthetically pleasing appearance.
At long-term follow-up, the patient showed significant improvement in body shape between the waist and knees. The thigh implants complemented the buttock implants, producing a more proportionate and aesthetically pleasing appearance.
Discussion
Buttock implants are well established in patients lacking adequate donor fat for BBL. Thigh implants, by contrast, are far less recognized but can be equally transformative. Like calf implants for the lower leg, thigh implants are placed on top of the muscle beneath the fascia. The difference is that thigh implants are considerably larger in both length and width, corresponding to the greater muscle mass of the upper leg.
Although not widely known, thigh implants have proven to be highly effective with low complication rates. As demonstrated in this case, their synergistic use with buttock implants offers excellent results in properly selected patients.
Key Points
- In men with flat buttocks and skinny legs, combined buttock and thigh implants can be performed during the same surgery.
- Intramuscular buttock implants are best for thin male patients to reduce the risks of visibility and malpositioning.
- Thigh implants are placed subfascially over the biceps femoris and vastus lateralis muscles to achieve anterolateral upper-leg augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon