

Jaw angle implant removal: Medpor vs silicone

|
Factor |
Medpor jaw angle implant |
Silicone jaw angle implant |
|
Tissue reaction |
Fibrovascular ingrowth into pores |
Smooth capsule around implant |
|
Plane of removal |
Often obliterated |
Usually preserved |
|
Removal method |
Sharp dissection, often piecemeal |
Usually en bloc extraction |
|
Operative difficulty |
High |
Low to moderate |
|
Masseter involvement |
Common integration into masseter/periosteum |
Usually displaced by capsule, not ingrown |
|
Bleeding |
More likely due to vascular ingrowth |
Usually less |
|
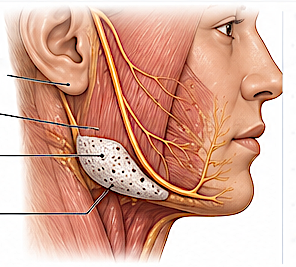
Marginal mandibular nerve risk |
Higher, especially if dissection exits deep plane |
Lower, but still possible |
|
Implant fragmentation |
Possible; retained fragments may occur |
Uncommon |
|
Bone surface after removal |
More irregularity/resorption possible |
Smooth pocket more common |
|
Post-removal contour deficit |
More likely |
Less dramatic, unless implant was large |
|
Reconstruction need |
Common; fat grafting, sling repair, new implant |
Less common; replacement easier |
|
Recovery |
More swelling, bruising, trismus |
Usually faster |
|
Revision predictability |
Less predictable |
More predictable |
Practical difference
Silicone jaw angle implant removal is usually a “find the capsule, open the pocket, remove the implant” operation.
Medpor jaw angle implant removal is more like “re-enter scarred tissue, protect the facial artery, cut the implant free from ingrown soft tissue, remove it in pieces, then manage the contour defect.”
Key surgical implication
With silicone, the priority is usually complete removal and pocket management.
With Medpor, the priority is:
Artery and muscle preservation > soft tissue preservation > complete removal > contour reconstruction
So a tiny retained Medpor fragment may be safer than aggressive dissection near the facial artery.
Dr Barry Eppley
Plastic Surgeon