

The treatment of frontal-based migraines by supraorbital and supratrochlear nerve decompression (stripping the muscle away from the nerves) has made a significant contribution to improved results for well qualified patients. (positive Botox responders)While it does not always cure every patient, numerous studies support that migraine headache frequency and severity are decreased in the majority of patients by this approach.
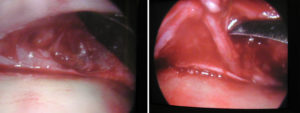 While the supraorbital and supratrochlear nerves course through muscle on their way up through the forehead tissues, there is a bony exit or foramen where it exits the brow bone of the frontal skull. As the nerve comes out of the bone, it is well known that there is a variety of shapes including an encircled complete bony foramen, a notch at the lower edge of the brow bone or some combination of both. This is also a potential source of nerve compression as a non-muscular trigger and is worthy of additional evaluation.
While the supraorbital and supratrochlear nerves course through muscle on their way up through the forehead tissues, there is a bony exit or foramen where it exits the brow bone of the frontal skull. As the nerve comes out of the bone, it is well known that there is a variety of shapes including an encircled complete bony foramen, a notch at the lower edge of the brow bone or some combination of both. This is also a potential source of nerve compression as a non-muscular trigger and is worthy of additional evaluation.
In the December 2012 issue of Plastic and Reconstructive Surgery, this relationship is studied in the article ‘The Anatomical Morphology of the Supraorbital Notch: Clinical Relevance to the Surgical Treatment of Migraine Headaches’. The bilateral supraorbital nerve exits in 30 cadaver heads were studied. In just over ¼ of the nerves, it came out through a foramen above the edge of the brow bone. In the majority (83%), the nerve was associated with a notch. Only 10% had a combination of a foramen and a notch. Interestingly, some nerves showed differences (foramen vs notch) between the two sides in the same head. When a notch was present, there was a fascial band that encircled the bottom part of the nerve most of the time. (86%) The authors identified four types of supraorbital notch bands based on their fascial and bony compositions.
This study is extremely relevant for the treatment of frontal migraines as it has identified for the first time in detail potential proximal compression points at the supraorbital nerve exit. This suggests that when there is a supraorbital notch present (which can even be identified prior to surgery by palpation) its complete release should be done or at least considered. The best way to ensure complete notch release is the ability to move the nerve away from the notch in both right and left directions. Whether such fascial releases are truly beneficial seems logical as that is part a fundamental component of decompressions of numerous other nerve surgeries for chronic pain and sensory dysfunction.
Dr. Barry Eppley
Indianapolis, Indiana