

A complete flat back of the head (often called occipital flatness or brachycephaly) can be augmented surgically if someone wants a more rounded, balanced skull shape. This is a real and fairly specialized area of craniofacial / aesthetic skull surgery.
What is skull (occipital) augmentation?
It’s a cosmetic procedure that adds projection and roundness to the back of the head by increasing skull contour. Hair covers the incision, so the change is shape-based rather than “scar-based.”
Main surgical options
1. Custom solid implant (most common & most precise)
Best option for most adults
- A custom-designed implant (usually silicone or Medpor) is made from a 3D CT scan
- Designed to correct flatness, asymmetry, or widen/narrow the back of the head
- Placed directly on the skull bone under the scalp
Pros
- Very precise shape control
- Immediate, predictable results
- Permanent
Cons
- Implant-related risks (low but real)
This is the gold standard for aesthetic skull reshaping.
2. Bone cement (PMMA) augmentation
Less commonly used today
- Surgeon sculpts bone cement directly onto the skull
- Hardens in place
Pros
- No prefabricated implant
- Costs less
Cons
- Far less precise than custom implants
- Requires longer scalp incision
- Harder to revise
- Prone to irregularities/asymmetry
- Limited augmentation effect (less than 60ccs)
- More surgeon-dependent result
3. Fat grafting
Usually not effective for the back of the head
- Fat resorbs unpredictably
- Can’t create firm, structural projection
- Rarely gives visible long-term improvement
Incision & recovery
- Incision: hidden in the hair (often low occipital)
- Surgery time: 1.5 to 2 hours
- Outpatient or overnight
- Swelling: 2–3 weeks
- Return to normal activity: ~2–3 weeks
- Final shape: visible immediately, refined over weeks
Hair can be washed within a few days, and scars are typically invisible once healed.
Who is a good candidate?
? Adults with:
- Naturally flat occiput
- Asymmetry from childhood positioning
- Desire for better head shape balance (often noticed in photos, haircuts, helmets, or glasses fit)
? Not ideal if:
- Unrealistic expectations about head size. This is avoided by preoperative imaging to establish potential outcomes
Risks (uncommon but important)
-
Infection
- Scalp numbness (usually temporary)
- Seroma or fluid buildup
With experienced surgeons, complication rates are low.
Aesthetic impact
Patients often report:
- Better head shape in profile
- Hair sits more naturally
- Improved overall head–neck balance
- Increased confidence (especially in photos)
Case Study
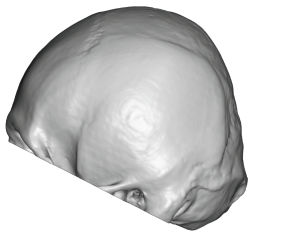
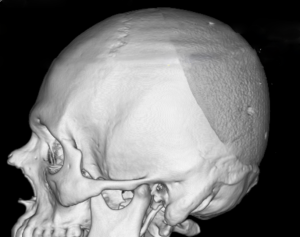
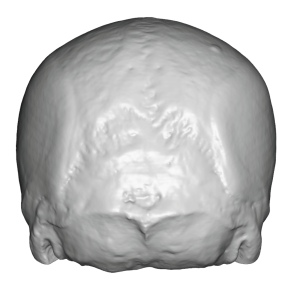 This male had a very flat back of the head for a significant brachycephaly profile. His lack of occipital projection had a central area that projected less than that of the posterior temporal lines. This resulted in a decreased width between the posterior temporal lines.
This male had a very flat back of the head for a significant brachycephaly profile. His lack of occipital projection had a central area that projected less than that of the posterior temporal lines. This resulted in a decreased width between the posterior temporal lines.
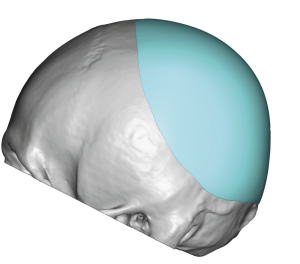
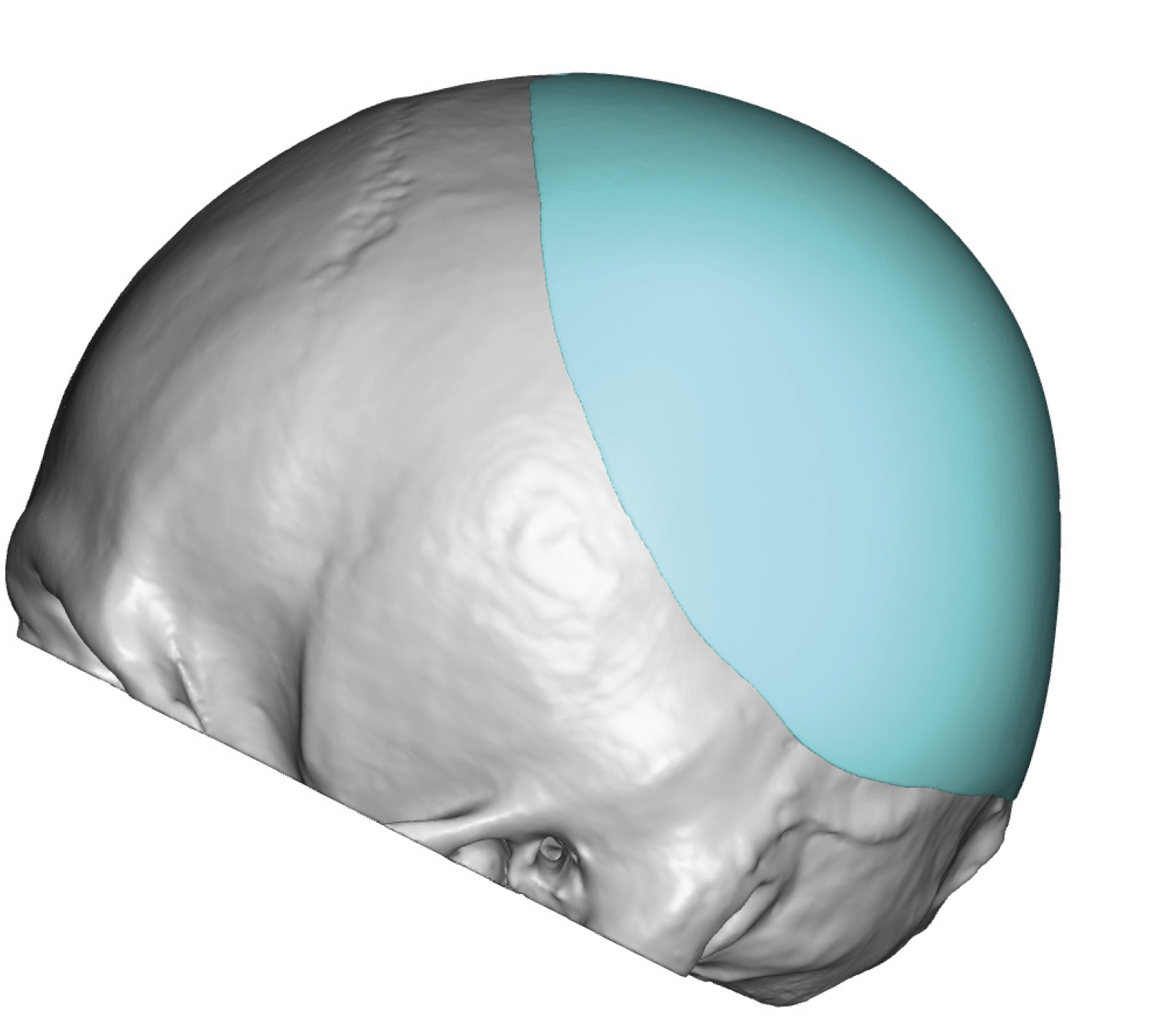
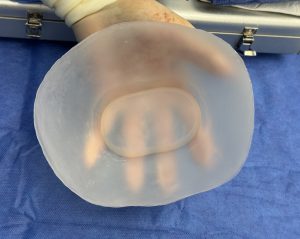
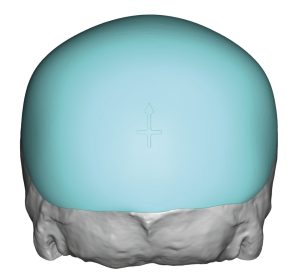 A custom back of the head implant was designed for maximal augmentation based on a safe estimate of scalp stretch with 15mm projection and 155cc volume. To aid placement via finding of the implant a inner racetrack relief of material was placed in the undersurface of the implant.
A custom back of the head implant was designed for maximal augmentation based on a safe estimate of scalp stretch with 15mm projection and 155cc volume. To aid placement via finding of the implant a inner racetrack relief of material was placed in the undersurface of the implant.
 In the prone position in surgery the extreme flatness of the back of his head could be demonstrated by the ‘cup test’ where the flat bottom of a cup sits stable on the occiput.
In the prone position in surgery the extreme flatness of the back of his head could be demonstrated by the ‘cup test’ where the flat bottom of a cup sits stable on the occiput.
 Through a low scalp incision placed over the nuchal ridge the custom occipital skull implant was placed a secured aided by the inner relief on the implant.
Through a low scalp incision placed over the nuchal ridge the custom occipital skull implant was placed a secured aided by the inner relief on the implant.

 When seen after surgery the immediate effects of the implant could be seen with increased projection but with a natural shape.
When seen after surgery the immediate effects of the implant could be seen with increased projection but with a natural shape.
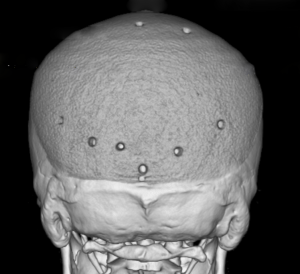 A post op 3D CT scan showed the positioning of the implant which is as close to ideal as could be surgically achieved.
A post op 3D CT scan showed the positioning of the implant which is as close to ideal as could be surgically achieved.
Discussion
In any form of skull augmentation, including occipital augmentation, millimeters matter. In my experience these are realistic typical occipital projection ranges (in mm).
Mild flatness correction
? 4–6 mm
- Subtle rounding
- Often enough to remove the “flat spot”
- Usually not noticeable to others, but felt by the patient
- Conservative augmentation
Think refinement, not size change.
Moderate augmentation
? 7–10 mm
- Clearly improves profile and head shape
- Makes hair sit better and rounder
- Noticeable in side photos
- Still very natural-looking
This is the sweet spot for most adults.
Significant augmentation
? 11–15 mm
- Used for pronounced flatness or brachycephaly
- Clearly changes head silhouette
- Often combined with lateral widening or vertical height
- Needs careful design so it doesn’t look “added on.”
Large / aggressive augmentation
? 16–20+ mm
- Usually requires 1st stage scalp expansion
- Needs careful design so it doesn’t look ‘added on’.
- The more backward projection they more it need to wrap around the sides and top to look natural.
What limits projection?
1Scalp tightness (biggest limiter)
- The scalp does not stretch easily which is magnified in naturally flatter head shapes
- More projection = greater scalp tension
Implant footprint
Projection is rarely just a “bump”:
- Good implants spread volume over a wide surface area
- Wider footprint = safer, more natural projection
How surgeons decide the number
Surgeons don’t just pick a number — they:
- Review CT scan
- Simulate multiple implant thicknesses
- Evaluate scalp tolerance
- Balance projection with width and height
Many surgeons will intentionally under-augment by ~1–2 mm for safety and natural appearance.
What patients usually think vs reality
Most patients come in thinking they need:
“At least 15–20 mm”
Most end up happiest with:
8–10 mm
Because the human eye reads curvature, not raw thickness.
Dr Barry Eppley
Plastic Surgeon