

Augmentation of the complete lower jaw, more commonly referred to as a custom jawline implant, is one of the most frequently requested custom implants particularly in the younger male. While standard chin and jaw angles implants can be used for the same intended purpose, they are less effective at achieving the complete jawline augmentation effect in a controlled and predictable manner. Thus the popularity of a creating an individual design for the many variabilities in anatomic shapes and aesthetic desires amongst patients.
 This is not to say that the use of performed chin and jaw angle implants can never work effectively in some patients because they can. But what makes the custom jawline implant so compelling is the linear connectivity of it, which due to the surface area coverage, has a more powerful effect at reshaping the lower third of the face. This is of particular interest in men who want to have an overall stronger and well defined jawline. It is also effective forwomen who seek a linear jawline look. But they usually have different shape objectives which is that of being tapered frontally but with a distinct jaw angle appearance.
This is not to say that the use of performed chin and jaw angle implants can never work effectively in some patients because they can. But what makes the custom jawline implant so compelling is the linear connectivity of it, which due to the surface area coverage, has a more powerful effect at reshaping the lower third of the face. This is of particular interest in men who want to have an overall stronger and well defined jawline. It is also effective forwomen who seek a linear jawline look. But they usually have different shape objectives which is that of being tapered frontally but with a distinct jaw angle appearance.

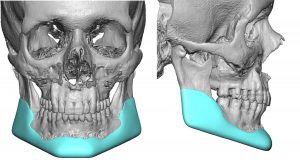
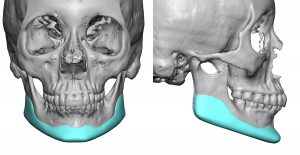
 In designing custom jawline implants the dimensions and shapes of the three corners (chin and jaw angles) must be taken into consideration along with how they are all connected across the true linear gap between them. (body of the mandible) Unfortunately creating such implant designs is not an exact science (yet) and a gap remains between fully appreciating how the designed size and shape of the implant correlates with the patient’s exact aesthetic desires. It takes a lot of experience to learn the nuances of these implant designs. But one overwhelming design oversight for patients and novice surgeons is the failure to appreciate the effects of an implant that covers such a large bony surface area. Traditional perceptions of linear measurements and thickness that come from using standard smaller facial implants take on a different significance. It is easy to design a jawline implant that ends up being too big. Typical custom jawline implant volumes will be in the range of 14 to 18ccs. Such effects can make a profound difference in the shape of the lower face.
In designing custom jawline implants the dimensions and shapes of the three corners (chin and jaw angles) must be taken into consideration along with how they are all connected across the true linear gap between them. (body of the mandible) Unfortunately creating such implant designs is not an exact science (yet) and a gap remains between fully appreciating how the designed size and shape of the implant correlates with the patient’s exact aesthetic desires. It takes a lot of experience to learn the nuances of these implant designs. But one overwhelming design oversight for patients and novice surgeons is the failure to appreciate the effects of an implant that covers such a large bony surface area. Traditional perceptions of linear measurements and thickness that come from using standard smaller facial implants take on a different significance. It is easy to design a jawline implant that ends up being too big. Typical custom jawline implant volumes will be in the range of 14 to 18ccs. Such effects can make a profound difference in the shape of the lower face.

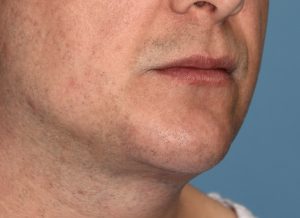 While the effect of a custom jawline implant can provide substantial mandibular augmentation, its definition will only be as visible as the thickness of the overlying soft tissues will permit. It is very much like covering a small ball with a sheet or a quilt…which one shows the shape of what underlies it better? Thus, combining jawline augmentation with soft tissue reduction procedures (buccal lipectomy, perioral liposuction, neck liposuction, submentoplasty) may be necessary in some patients.
While the effect of a custom jawline implant can provide substantial mandibular augmentation, its definition will only be as visible as the thickness of the overlying soft tissues will permit. It is very much like covering a small ball with a sheet or a quilt…which one shows the shape of what underlies it better? Thus, combining jawline augmentation with soft tissue reduction procedures (buccal lipectomy, perioral liposuction, neck liposuction, submentoplasty) may be necessary in some patients.
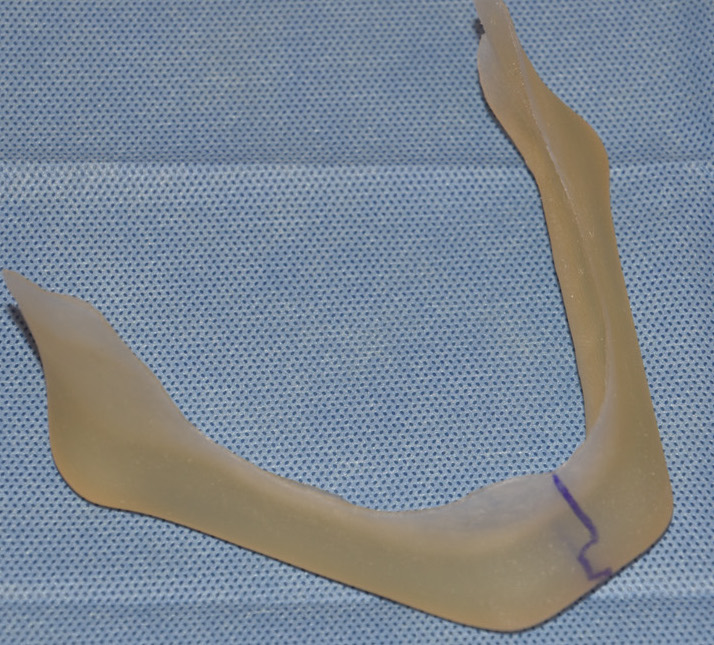
A custom wrap-around jawline implant is almost always inserted through three separate incisions. (two posterior intraoral and one anterior submental/intraoral) Through these small and separated incisions the large implant must the inserted and positioned. It sounds easy…but it isn’t. Once inside the pocket less than 50% oft the implant can be fully visualized and the exact positioning on the bone is much harder to determine than one would think particularly in the critical jaw angle areas. Insertion of the implant can be done in a front to back method if the jaw angles of the implant are not too big. If the jaw angles are too thick to be folded on insertion to pass under the mental nerve, a split implant technique is used. The implant is separated at the chin area in a geometric split technique and then is inserted in a back to front technique going from inside the mouth. The implant is then reassembled in the midline once inside the pocket.
Regardless of how the implant is inserted the insertion technique it is critically important to use screw fixation at the chin and jaw angle areas. At the chin either self-drilling 2.0mm or drilled 2.0mm screws can be used based on the thickness of the implant. At the jaw angles 2.0mm self-drilling screws are placed using a percutaneous technique. The screwdriver is passed externally through the tissues in a perpendicular fashion using a 2mm skin nick incision. This allows the screws to be placed in a more secure perpendicular fashion rather than at more precarious angles to the implant and bone when attempted intraorally.
Dr. Barry Eppley
Indianapolis, Indiana