

The treatment of undereye hollows has become commonplace with the widespread use of synthetic fillers and fat injections. While providing a solution for these aesthetic undereye concerns, such injection therapies are not perfect. Besides the lack of permanence for either fillers or fat, irregularities and contour issues from the added volume creates a need for more assured aesthetic outcomes that persist.
 One such implant solution is the use of preformed tear trough implants. While perhaps effective for the isolated tear trough deformity, many undereye hollows require a combined horizontal and vertical infraorbital rim augmentation. (implant saddle effect) Therein lies the limitations of preformed tear trough implants which can only provide horizontal augmentation, thus creating an incomplete infraorbital rim enhancement. Adequate undereye correction must also include a vertical elevation of the infraorbital rim in many patients. Only a custom infraorbital rim implant design can provide adequate volumetric fill in all three dimensions of the undereye area..
One such implant solution is the use of preformed tear trough implants. While perhaps effective for the isolated tear trough deformity, many undereye hollows require a combined horizontal and vertical infraorbital rim augmentation. (implant saddle effect) Therein lies the limitations of preformed tear trough implants which can only provide horizontal augmentation, thus creating an incomplete infraorbital rim enhancement. Adequate undereye correction must also include a vertical elevation of the infraorbital rim in many patients. Only a custom infraorbital rim implant design can provide adequate volumetric fill in all three dimensions of the undereye area..
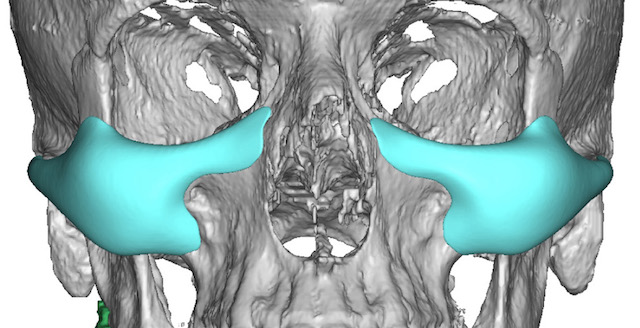
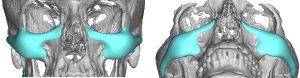 For patients with combined infraorbital rim recession and flatter cheeks (infraorbital malar hypoplasia) which commonly occur together and create a negative orbital vector, there is no standard implant that can adequately address both contiguous areas as a single implant. Efforts have been made to combine preformed tear trough and cheek implants to create this effect. But having two implants that do not connect and fails to cover all deficient bone surfaces has its aesthetic limitations. A custom implant design that provides adequate infraorbital rim coverage, both horizontally and vertically, with a snug fit to the bone and a malar extension that turns the corner onto the cheekbone and zygomatic arch is what is needed. Such a custom infraorbital-malar implant also feathers into the medial and lateral orbital rim areas without creating palpable or visible step-offs. The malar extension is what most effectively corrects the negative orbital vector as well as provides a smooth transition onto the side of the midface. How far back along the zygomatic arch the implant goes depends on whether lateral facial width is desired. It can stop short and have a feathered edge at the posterior end of the zygomatic body or extend all the way to the zygomatic process of the temporal bone.
For patients with combined infraorbital rim recession and flatter cheeks (infraorbital malar hypoplasia) which commonly occur together and create a negative orbital vector, there is no standard implant that can adequately address both contiguous areas as a single implant. Efforts have been made to combine preformed tear trough and cheek implants to create this effect. But having two implants that do not connect and fails to cover all deficient bone surfaces has its aesthetic limitations. A custom implant design that provides adequate infraorbital rim coverage, both horizontally and vertically, with a snug fit to the bone and a malar extension that turns the corner onto the cheekbone and zygomatic arch is what is needed. Such a custom infraorbital-malar implant also feathers into the medial and lateral orbital rim areas without creating palpable or visible step-offs. The malar extension is what most effectively corrects the negative orbital vector as well as provides a smooth transition onto the side of the midface. How far back along the zygomatic arch the implant goes depends on whether lateral facial width is desired. It can stop short and have a feathered edge at the posterior end of the zygomatic body or extend all the way to the zygomatic process of the temporal bone.
 Infraorbital or combined infraorbital-malar implants are most reliably placed through a lower eyelid approach. Isolated infraorbital rim implants can be placed through a transconjunctival incision but more extended designs require a subciliary lower eyelid incision. A few millimeters of a lateral canthal skin extension with a hemi- or partial lower eyelid incision (lateral half of the lower eyelid) is all that is usually needed. A good supportive closure (cheek soft tissue and orbicularis muscle resuspension with lateral canthopexy) ensures a discrete lower eyelid scar line and good postoperative apposition of the lid to the globe. Such lower eyelid incisions heal better and have lower risks than the traditional lower blepharoplasty incision in the older patient as no tissue is removed and the implant provides improved lower eyelid support.
Infraorbital or combined infraorbital-malar implants are most reliably placed through a lower eyelid approach. Isolated infraorbital rim implants can be placed through a transconjunctival incision but more extended designs require a subciliary lower eyelid incision. A few millimeters of a lateral canthal skin extension with a hemi- or partial lower eyelid incision (lateral half of the lower eyelid) is all that is usually needed. A good supportive closure (cheek soft tissue and orbicularis muscle resuspension with lateral canthopexy) ensures a discrete lower eyelid scar line and good postoperative apposition of the lid to the globe. Such lower eyelid incisions heal better and have lower risks than the traditional lower blepharoplasty incision in the older patient as no tissue is removed and the implant provides improved lower eyelid support.
Dr. Barry Eppley
Indianapolis, Indiana