

Bringing the midface forward is often a desire from patients with an overall flatter midface profile. Such lack of midface projection may be present naturally (e.g., some Asian faces although it can occur in any ethnicity), may be present after trauma or may be persistent after a prior Lefort I ostetotomy. (incomplete midface correction) It is a result of lack of skeletal development anteriorly of the maxilla, infraorbital rims and anterior cheeks as a collective unit.
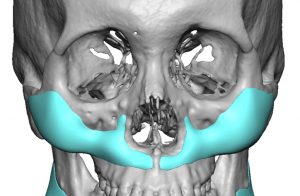
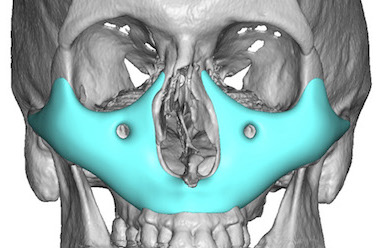
 While once thought that creating partial or total midface projection could only be done by various types of LeFort osteotomies, custom midface implant designs allow for a less invasive and more controlled method of doing so. (minus any occlusal change) The entire midface can be augmented from the infraorbital rims down to just above the maxillary alveolus. There are a variety of midface implant designs that can be done based on the patient’s anatomic needs. When covering the entire midface this is known as the midface mask implant.
While once thought that creating partial or total midface projection could only be done by various types of LeFort osteotomies, custom midface implant designs allow for a less invasive and more controlled method of doing so. (minus any occlusal change) The entire midface can be augmented from the infraorbital rims down to just above the maxillary alveolus. There are a variety of midface implant designs that can be done based on the patient’s anatomic needs. When covering the entire midface this is known as the midface mask implant.

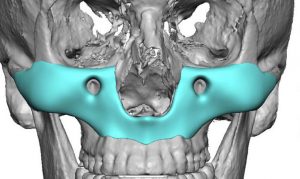
 Such custom midface implants are placed through an intraoral approach, sometimes as one piece and others as a split implant technique based on its size. To avoid creating a complete block of the bone from the overlying soft tissues, I think it is biologically sound to create perfusion in the implant at the time of surgery. Such holes in the implant creates the ability for the body to re-establish a soft to bone vascular connection at various hole locations.
Such custom midface implants are placed through an intraoral approach, sometimes as one piece and others as a split implant technique based on its size. To avoid creating a complete block of the bone from the overlying soft tissues, I think it is biologically sound to create perfusion in the implant at the time of surgery. Such holes in the implant creates the ability for the body to re-establish a soft to bone vascular connection at various hole locations.
Another intraoperatve helpful maneuver is to increase the soft thickness over the implant. This can be done using the buccal pads in a pedicled transposition technique to cover the implant and provide an additional vascularized soft tissue layer between the mucosal closure and the underlying implant. This also adds some soft tissue fullness which helps the projection.The buccal fat pads can be teased out and usually creates a long enough pedicle flap to reach the midline from each side.
Dr. Barry Eppley
Indianapolis, Indiana