

Hollows under the eyes occur for a variety of aging and development reasons. As one ages tissues thin and fat atrophies and the once fuller lower eyelid region can become more sunken. In other patients the support under the lower eyelid, the infraorbital bone, lacks good development and a natural hollowing has always existed. Aging will accentuate this congenital lack of good infraorbital bone projection as tissue atrophy magnifies it.
Infraorbital hollows must be differentiated in its origin as this impacts potential treatments. Those caused by age-related soft tissue atrophy can be managed by a variety of soft tissue strategies from injectable fillers and fat to open eyelid approaches from fat transposition and the placement of soft tissue grafts.

 But infraorbital hollows caused by a bone deficiency are best treated by a bone augmentation approach. These are evident by the classic negative orbital vector and generalized recession under the eye and extending out into the anterior cheek. The best bone-based treatment is that of a custom infraorbital implant. Designed off of the patient’s 3D CT scan, its design saddles the infraorbital rim as opposed to the traditional off-the-shelf tear trough implant which is placed on the front edge of the infraorbital rim. This may seem like a subtle distinction but it is not. This is because such lower orbital bone deficiencies are multi-dimensional, meaning it is usually a combined vertical and horizontal deficiency. It is important to raise up the vertical level of the infraorbital rim as well as bring it forward.
But infraorbital hollows caused by a bone deficiency are best treated by a bone augmentation approach. These are evident by the classic negative orbital vector and generalized recession under the eye and extending out into the anterior cheek. The best bone-based treatment is that of a custom infraorbital implant. Designed off of the patient’s 3D CT scan, its design saddles the infraorbital rim as opposed to the traditional off-the-shelf tear trough implant which is placed on the front edge of the infraorbital rim. This may seem like a subtle distinction but it is not. This is because such lower orbital bone deficiencies are multi-dimensional, meaning it is usually a combined vertical and horizontal deficiency. It is important to raise up the vertical level of the infraorbital rim as well as bring it forward.
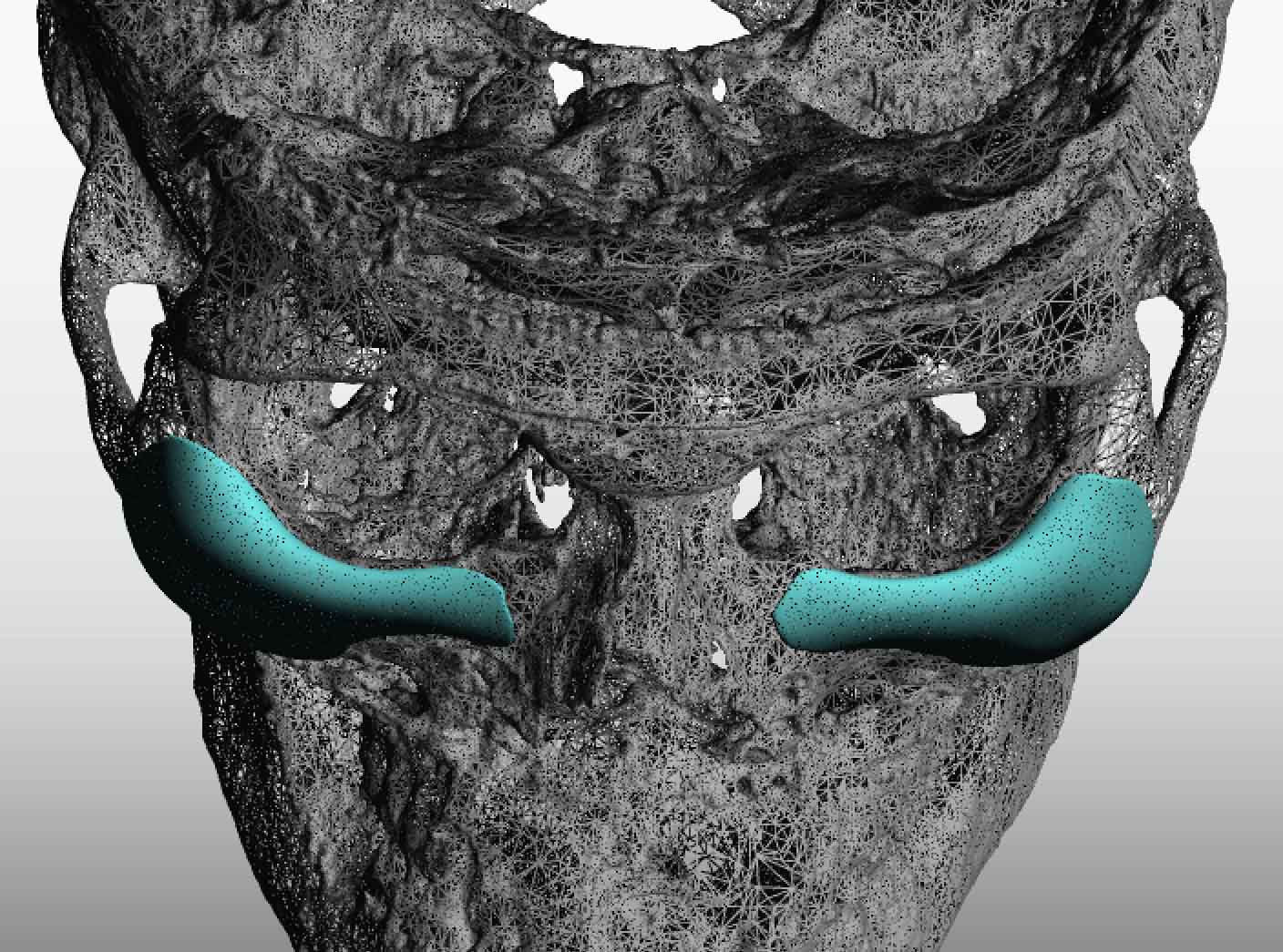
 Infraorbital rim deficiency rarely occur in isolation since their development is part of the ZMC or zygomatico-maxillary-orbital complex. This explains why the cheek is flat in many bone-based lower eye hollows. As a result an implant design may not be isolated to the infraorbital rim only. It may need to extend out onto the anterior cheek/upper maxilla. How far it should go depends the degree of cheek augmentation the patient seeks if any. This is known as the infraorbital-malar implant design. If not the design can stop at the outer edge of upper anterior cheek.
Infraorbital rim deficiency rarely occur in isolation since their development is part of the ZMC or zygomatico-maxillary-orbital complex. This explains why the cheek is flat in many bone-based lower eye hollows. As a result an implant design may not be isolated to the infraorbital rim only. It may need to extend out onto the anterior cheek/upper maxilla. How far it should go depends the degree of cheek augmentation the patient seeks if any. This is known as the infraorbital-malar implant design. If not the design can stop at the outer edge of upper anterior cheek.
Custom infraorbital implants are placed through a lower eyelid incision for best placement and positioning on the bone. I usually secure it with two microscrews per side to ensure standard stability. Lower eyelid closure require soft tissue resuspension including the cheek tissues and orbicularis muscle suspension to the periosteum of the bone.
Dr. Barry Eppley
Indianapolis, Indiana