

One of the common questions I get in regards to custom infraorbital-malar (IOM) implants is can they be placed through an intraoral approach. This question is asked because most of the time I do place them through a lower eyelid incision. Having placed them earlier in my clinical experience through the intraoral route I can comment on the merits of either placement pathway.
Since a custom infraorbital-malar implant is a variation of a cheek implant it is logical to assume that it can similarly be placed. The question is not whether it can be placed intraorally but whether it should and are there increased risks by doing so.
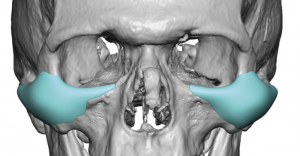 That question is answered by looking at the difference between a standard cheek implant and the IOM implant. While the cheek implant is largely differing variations of an oval, the IOM implant is more longitudinal in shape. This is because of its infraorbital and zygomatic arch extensions. This shape distinction is what separates them in regards to two key elements, getting proper implant placement on the bone and the risk of infraorbital nerve dysesthesia.
That question is answered by looking at the difference between a standard cheek implant and the IOM implant. While the cheek implant is largely differing variations of an oval, the IOM implant is more longitudinal in shape. This is because of its infraorbital and zygomatic arch extensions. This shape distinction is what separates them in regards to two key elements, getting proper implant placement on the bone and the risk of infraorbital nerve dysesthesia.
Oval shaped cheek implants are positioned lateral to the infraorbital nerve and their placement largely overlies that of the cheekbone proper. Thus coming from the intraoral route is the most direct method of placement and there is reasonable visualization of a significant portion of the implant on the bone.
 In contrast many IOM implant designs have long anterior and posterior wings (the infraorbital and arch components) where intraoral visibility of their placement is more limited. Some infraorbital rim access can be obtained intraorally but it is necessary to work around the infraorbital nerve. If there isn’t much of an infraorbital component this is not a major issue. But if the IOM implant covers the entire rim and saddles it in any way there is no visibility when coming from below to ensure good placement. As for the zygomatic arch there is no visibility at all from the intraoral approach and the path of dissection is very poorly visualized if at all.
In contrast many IOM implant designs have long anterior and posterior wings (the infraorbital and arch components) where intraoral visibility of their placement is more limited. Some infraorbital rim access can be obtained intraorally but it is necessary to work around the infraorbital nerve. If there isn’t much of an infraorbital component this is not a major issue. But if the IOM implant covers the entire rim and saddles it in any way there is no visibility when coming from below to ensure good placement. As for the zygomatic arch there is no visibility at all from the intraoral approach and the path of dissection is very poorly visualized if at all.
 When coming from the lower eyelid approach in an IOM implant, the infraorbital rim is completely visualized. While the zygomatic arch beyond the mid-zygomatic suture line can not be seen the path of dissection is longitudinal right along the line of the arch. As a result the risk of IOM implant malposition is much lower than when trying to do so from the mouth. In addition all the dissection is done above the infraorbital nerve so the risk of dysesthesia is negligible.
When coming from the lower eyelid approach in an IOM implant, the infraorbital rim is completely visualized. While the zygomatic arch beyond the mid-zygomatic suture line can not be seen the path of dissection is longitudinal right along the line of the arch. As a result the risk of IOM implant malposition is much lower than when trying to do so from the mouth. In addition all the dissection is done above the infraorbital nerve so the risk of dysesthesia is negligible.
In conclusion the advantages of the lower eyelid incision for custom IOM implants is better placement, negligible risk of nerve injury and a lower infection risk. The risk of lower eyelid contracture/malposition is very different from that of a lower blepharoplasty given that no tissue is being removed and what is being implanted will make some contribution tower eyelid support.
Dr. Barry Eppley
Indianapolis, Indiana