

Chin implants are the most common form of facial implant augmentation. One of their most recognized features by x-rays are what is often described as ‘erosion’ or loss of bone underneath or around the implant. As a result it is a widely held belief that this is a pathologic phenomenon and bodes poorly for the jawbone, tooth roots and the implant itself.
 The concept of chin implant erosion comes from observations based on plain x-rays, particularly lateral or side profile images of the chin. But contemporary 3D CT scans allow for more in-depth insights into the type of bone reactions that occur around chin implants. Looking at thousands of 3D CT scan images that contain chin implants (in the design of custom chin and/or jawline implant replacements) combined with intraoperative observations of their removal allows for an improved understanding of the historically described ‘chin implant erosion’ phenomenon.
The concept of chin implant erosion comes from observations based on plain x-rays, particularly lateral or side profile images of the chin. But contemporary 3D CT scans allow for more in-depth insights into the type of bone reactions that occur around chin implants. Looking at thousands of 3D CT scan images that contain chin implants (in the design of custom chin and/or jawline implant replacements) combined with intraoperative observations of their removal allows for an improved understanding of the historically described ‘chin implant erosion’ phenomenon.
It is first important to recognize how all implants create their effects…soft tissue displacement. When a chin implant is placed on the bone its aesthetic effects come by pushing the overlying soft tissues outward creating an external contour change. But the overlying tissues do provide some pushback or recoil onto the implant initially. Because the implant violates the biologic boundaries by which the tissues were developed, and the implant itself can not change its structure, the tissue recoil or pressure effect on the implant is alleviated by the underlying tissues responding to it. And it does so by relieving the pressure through tissue adaptation or resorption around the implant. This is seen on plain x-rays in side view as the implant going into the bone. This is a passive phenomenon in which once the pressure is relieved and the biologic boundary is partially re-established the loss of bone ceases. No chin implant has ever been seen to settle completely through the bone or to go as deep as the implant thickness which demonstrates its self-limited effect. Because of the self-limiting nature of this tissue adaptation process it is better called ‘implant imprinting’.

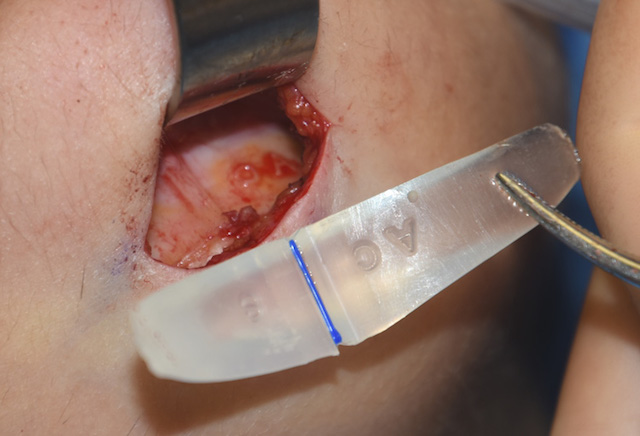
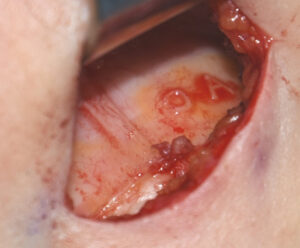 When looking carefully at the bone underneath a chin implant at its removal, it is seen as firm bone of normal consistency. An erosive or inflammatory process would cause soft abnormal bone that could be easily scraped off and removed. The implant-bone edges are distinct and firm. Every detail of the implant, including older chin implants that have letters for sizing and style on them, appear as crisp outlines on the bone.
When looking carefully at the bone underneath a chin implant at its removal, it is seen as firm bone of normal consistency. An erosive or inflammatory process would cause soft abnormal bone that could be easily scraped off and removed. The implant-bone edges are distinct and firm. Every detail of the implant, including older chin implants that have letters for sizing and style on them, appear as crisp outlines on the bone.
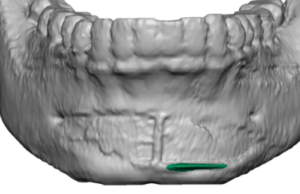
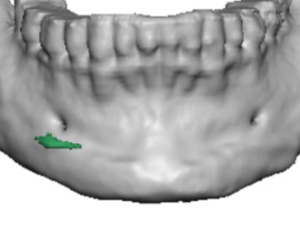
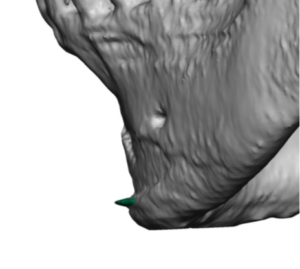 On 3D CT scans the impression of the implant on the bone is very clear, like it had been cut into the bone to fit like a puzzle piece. Bone will often be seen growing up around the implant edges. In rare cases I have seen an implant completely covered in a thin shell of bone. Such bone overgrowth is a result of elevation of the periosteum which can cause bone deposition that follows the surface of the implant. If an inflammatory process existed the bone edges would be neither so distinct nor would bone deposition occur around the implant edges.
On 3D CT scans the impression of the implant on the bone is very clear, like it had been cut into the bone to fit like a puzzle piece. Bone will often be seen growing up around the implant edges. In rare cases I have seen an implant completely covered in a thin shell of bone. Such bone overgrowth is a result of elevation of the periosteum which can cause bone deposition that follows the surface of the implant. If an inflammatory process existed the bone edges would be neither so distinct nor would bone deposition occur around the implant edges.
 Such chin implant imprinting is far more commonly seen when the plant is higher up on the bone where the cortical bone thickness is less. When the implant is placed down lower on the bone (where it is designed to be placed) imprinting is much less or does to occur at all. This may be because not only is the cortical bone thinner up higher but the pressure of the overlying mentalis muscle near its origin is greater.
Such chin implant imprinting is far more commonly seen when the plant is higher up on the bone where the cortical bone thickness is less. When the implant is placed down lower on the bone (where it is designed to be placed) imprinting is much less or does to occur at all. This may be because not only is the cortical bone thinner up higher but the pressure of the overlying mentalis muscle near its origin is greater.
Such chin implant imprinting is seen with all implant materials, it is not a biologic reaction just to solid silicone material. It is seen just as frequently with porous polyethylene (Medpor) and PEEK. Tissue ingrowth or an extremely firm material does not prevent it nor would it be expected to as the biologic adaptive effect of inserting an implant remains the same.
Implant imprinting is not restricted just to chin implants. I have seen it quite commonly at the jaw angles and cheeks as well. Jaw angle implant imprinting with bone overgrowth can be just as profound as that seen on the chin. Cheek implant imprinting seems to be much less visible perhaps due to the lack of a significant muscle presence/contraction over it unlike that of the chin (mentalis) and jaw angles. (masseter)
Dr. Barry Eppley
Indianapolis, Indiana