

One theory and approach to frontal migraine headaches has been the release of branches of the trigeminal nerve due to muscular and bony impingement. Whether pharmacologically treated by Botox injections or surgically treated by removal of constricting muscle and bone, dramatic and lasting improvements have been seen in properly selected patients.
One such treated area is that of the frontal migraine, commonly presenting as pain at the brow bone, behind the eye and up into the forehead. This is where the supraorbital and supratrochlear nerves exit the brow bone and can be entrapped by a tight bony foramen and/or the multiple muscles of the glabellar region. With adequate deompression, studies have shown that the majority of patients get lasting relief up to five years later with significant reduction in the frequency and intensity of their migraines.
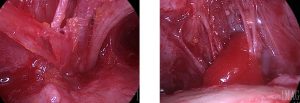 Surgical decompression of the frontal area can be performed by two basic approaches, either coming from above using an endoscope or approaching it from below through an upper eyelid incision. Having done it both ways I have often wondered does one approach produce better results than the other?
Surgical decompression of the frontal area can be performed by two basic approaches, either coming from above using an endoscope or approaching it from below through an upper eyelid incision. Having done it both ways I have often wondered does one approach produce better results than the other?
In the May 2012 issue of Plastic and Reconstructive Surgery, a study out of Case Western Reserve University in Cleveland Ohio addressed this very issue of surgical approach to frontal migraines. Such a published study is of particular interest since this institution and its senior author may be considered the father of modern-day migraine surgery. Based on retrospective reviews of over 250 patients who underwent frontal migraine surgery, nearly 80% of those that had an eyelid approach had a successful outcome (62 patients) compared to a near 90% successful outcome in those patients who were treated with an endoscopic approach. (191 patients) Slighty over half of the eyelid approach patients had complete elimination of their headaches while two-thirds of the endoscopic group did.
This paper makes the case that endoscopic treatment of frontal migraines is more effective. One reason is that a superior approach is more effective at removing the most amount of muscle in a 360 degree fashion around the nerves. Muscle access from the eyelid approach is partially blocked by the path of the nerves themselves often resulting inadequate resection. The authors also feel that the bony foramen or notch is much better located coming from above and this certainly is true based on my Indianapolis plastic surgery experience with cosmetic endoscopic browlift procedures.
The one limitation to endosocopic frontal migraine surgery is the length and shape of the forehead bone. A long forehead with a hairline that is 8cms or more from the brows make instrument access very difficult if not impossible. A similar limiting factor is if the forehead bone is very curved or prominent, again making instrument manipulation of the tissues around the nerves mechanically restricted.
Dr. Barry Eppley
Indianapolis, Indiana