

Background
The most common dimensional deficiency of the chin is inadequate forward projection, which is often well-corrected with an implant for modest augmentation. While horizontal projection is the most frequently treated deficiency, vertical chin deficiency is often underdiagnosed or overlooked. This is largely because most standard chin implants—except for one specialized type—only address horizontal augmentation. In many ways, the types of implants available influence how surgeons perceive and diagnose chin concerns.
Vertical chin deficiency is relatively easy to identify once one knows what to observe. The most obvious sign is a vertically short lower third of the face, as determined by the classic facial thirds assessment. Many patients with this condition also display a flat mandibular plane angle, where the jaw angles and chin align along nearly the same horizontal plane. However, the most definitive method of diagnosing vertical deficiency is through photographic imaging. By digitally simulating vertical chin lengthening, with or without simultaneous horizontal augmentation, patients can better appreciate the aesthetic benefits.
Treatment Considerations
Once the need for vertical chin lengthening is established, the question becomes how best to achieve it. For modest lengthening (up to 7 mm), an implant may suffice, as the soft tissue chin pad can still be stretched to cover the implant. However, vertical augmentation behaves very differently than horizontal augmentation. For instance, a 10 mm chin implant placed horizontally usually integrates well with the overlying soft tissue. Yet, if the same 10 mm increase is attempted vertically, the soft tissue pad often cannot fully drape over the implant. This leads to a “double bump” deformity, with the chin pad forming a higher bulge above the implant projection.
Therefore, more substantial vertical lengthening requires a bony lengthening technique. In this approach, the soft tissue chin pad remains attached to the underside of the chin and follows the repositioned bone downward, avoiding any separation or visible demarcation between soft tissue and bone.
Case Study
A female patient presented with a visibly short chin, confirmed both by facial thirds analysis and her own concerns. While she had a slight horizontal deficiency, her priority was vertical correction. Preoperative assessment determined she required at least 10 mm of vertical chin lengthening.
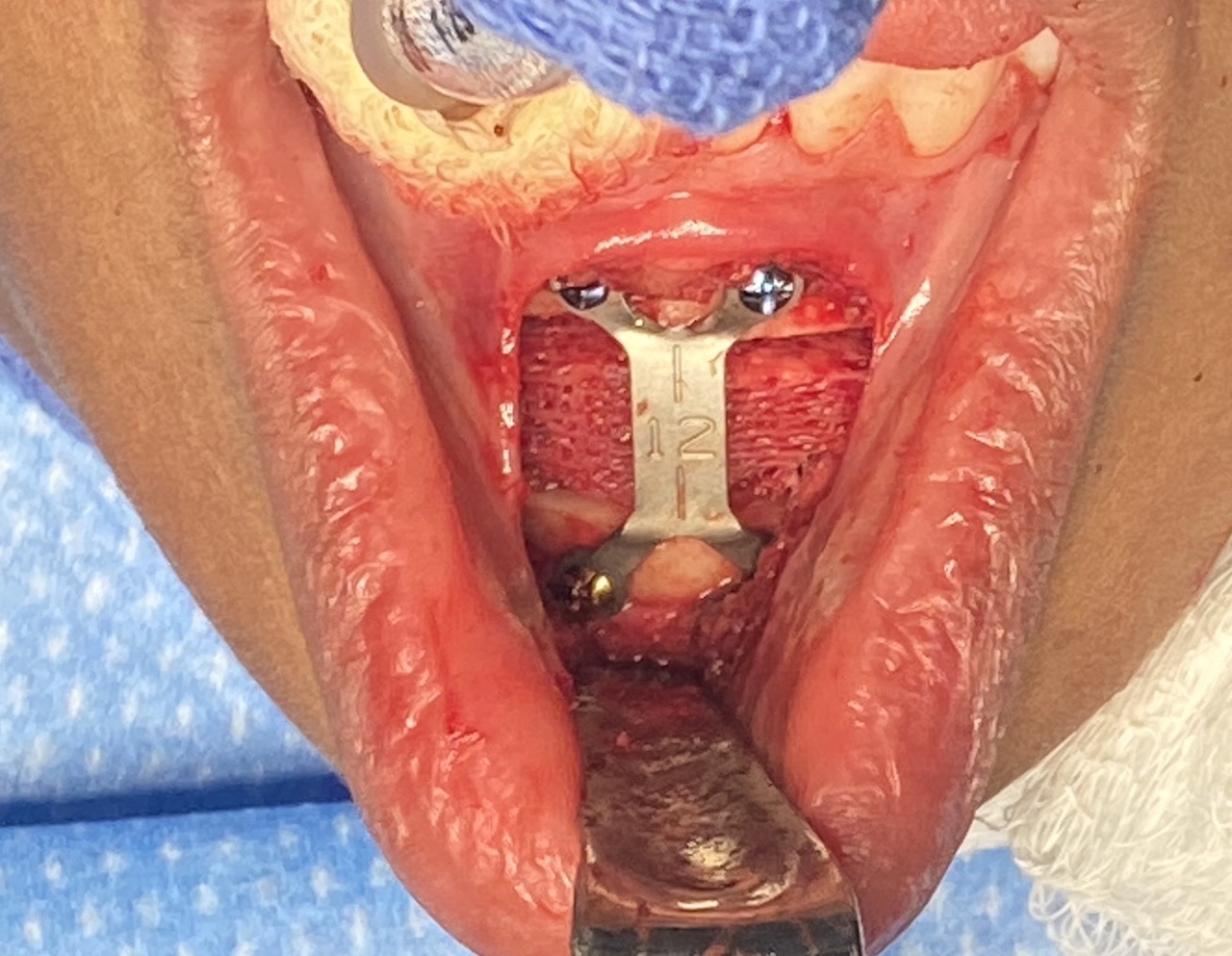
 Under general anesthesia, an intraoral approach was used to cut and reposition the chin bone. The chin was lowered 12 mm and stabilized with a fixation plate and screws. A cadaveric bone graft was inserted into the created gap.
Under general anesthesia, an intraoral approach was used to cut and reposition the chin bone. The chin was lowered 12 mm and stabilized with a fixation plate and screws. A cadaveric bone graft was inserted into the created gap.



 At two-year follow-up, the patient demonstrated a significantly improved lower facial proportion with sustained vertical chin lengthening. Importantly, her horizontal projection did not worsen. The bony lengthening method succeeded in creating a natural result because the chin pad maintained its attachment and descended seamlessly with the bone.
At two-year follow-up, the patient demonstrated a significantly improved lower facial proportion with sustained vertical chin lengthening. Importantly, her horizontal projection did not worsen. The bony lengthening method succeeded in creating a natural result because the chin pad maintained its attachment and descended seamlessly with the bone.
It should be noted that in pure vertical lengthening, the counterclockwise rotation of the osteotomized bone can also create some degree of horizontal projection. This effect becomes more pronounced when the vertical increase is 10 mm or greater and should be accounted for in surgical planning.
Key Points
-
Bony genioplasty provides the most effective correction for vertical chin deficiency.
-
A cadaveric corticocancellous bone graft is used to fill the interpositional gap created during vertical lengthening.
-
The wedge-opening osteotomy causes counterclockwise bone rotation, which may affect horizontal projection.
Dr. Barry Eppley
World-Renowned Plastic Surgeon