

There are many types of dimensional changes that can be done to the bony chin. From an osteotomy standpoint, the most common bony movement is horizontal of the down fractured segment with the well known sliding genioplasty procedure. This is effective at not only moving the bone but also has the benefit of moving the submental tissue beside and beneath it as well due to their bony attachments.
One of these tissue attachments is the geniohyoid muscle. This paired suprahyoid muscle originates from the bony spine on the backside of the chin bone and inserts back and down onto the hyoid bone below. When the bone is cut and downfractured for a sliding genioplasty, its attachment remains and the muscle is pulled forward as the chin is moved forward. This serves as the anatomic basis for an improved submental contour in the forward advancing sliding genioplasty.
But in vertical chin reductions done by the intraoral removal of a horizontal wedge of bone (wedge reduction genioplasty), the geniohyoid muscle is at risk. In removing the wedge of bone part or all of the genioglossus attachment may be lost. The retracted muscle can pull downward toward the hyoid and can create increased submental fullness.
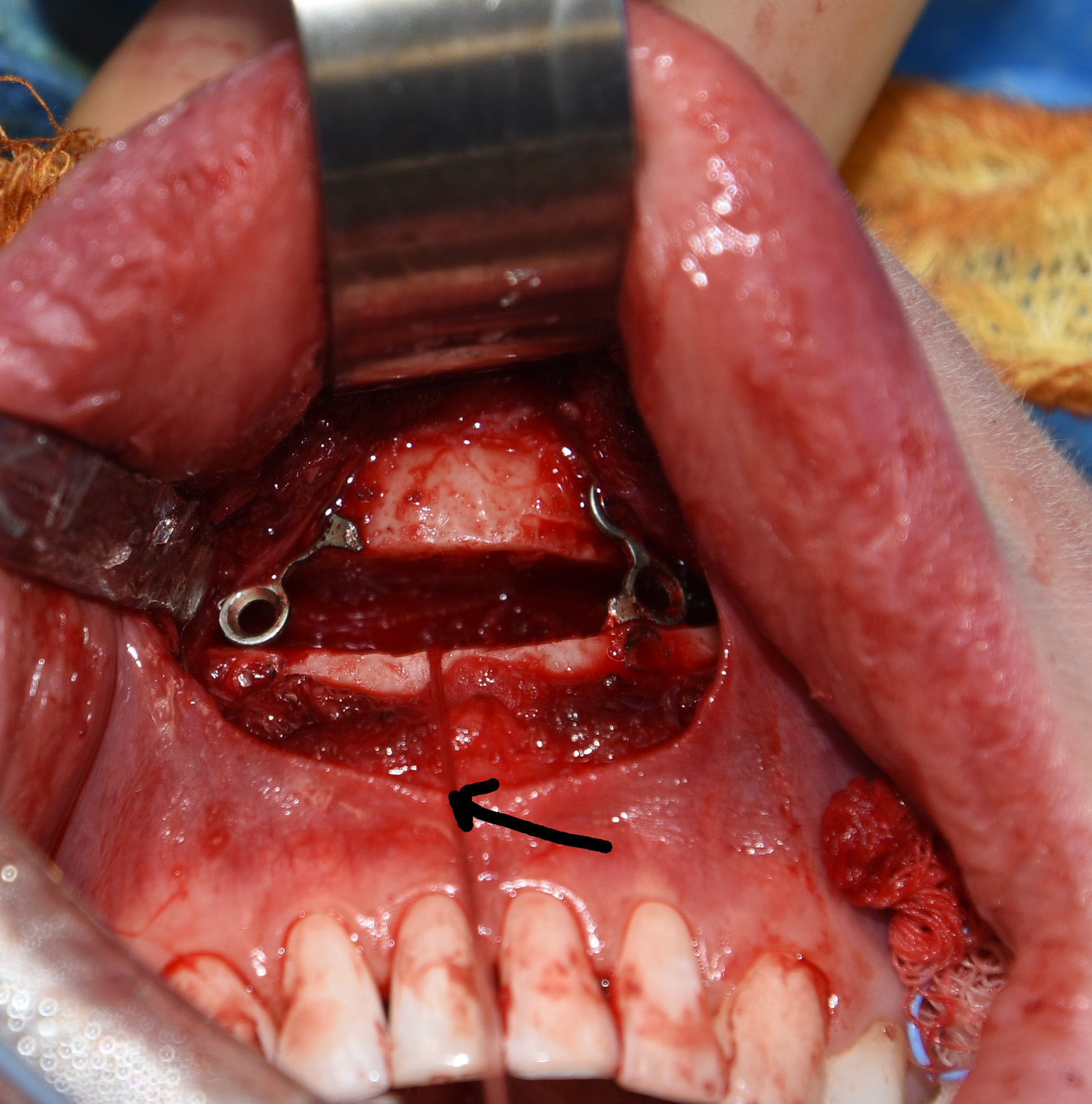 To prevent this muscle contraction possibility, the geniohyoid muscle attachment is removed from the wedge of bone and grasped with suture. This suture is kept in the midline and the downfractured bone segment is brought back up to close the space from the removed bone wedge. The bone is secured in its vertically shortened position with 1.5mm plates and screws. The muscle suture is then tied down to a single screw placed in the midline, creating a bone-anchored soft tissue attachment.
To prevent this muscle contraction possibility, the geniohyoid muscle attachment is removed from the wedge of bone and grasped with suture. This suture is kept in the midline and the downfractured bone segment is brought back up to close the space from the removed bone wedge. The bone is secured in its vertically shortened position with 1.5mm plates and screws. The muscle suture is then tied down to a single screw placed in the midline, creating a bone-anchored soft tissue attachment.
In vertical chin reduction any increased fullness of the submental region below it would be aesthetically disadvantageous. Keeping tensions across the geniohyoid muscle will help prevent that from occurring.
Dr. Barry Eppley
Indianapolis, Indiana