

The tear trough is a natural depression that runs from the inner aspect of the eye down along the infraobital rim, usually stopping at about a vertical line drawn down from the pupil of the eye. With aging, it becomes deeper and more visible and then becomes known as the tear trough deformity. Extending from the tear trough is another line known as the lid-cheek junction or palpebromalar groove. Both the tear trough and palpebromalar groove have drawn a lot of interest in reducing their presence primarily through the use of injectable fillers.
Currently there are two known methods for treating the tear trough deformity, injectable fillers and lower blepharoplasty surgery. By far injectable fillers are most commonly used because of their simplicity and immediate effects. But this is not a fool proof treatment and is prone to complications such as lumpiness and irregularities. The filler can be placed right under the skin or under the orbicularis muscle and each location has its own advantages and disadvantages.
 Surgical correction through a lower blepharoplasty can be done using a variety of techniques of which the most effective are orbital fat repositioning and orbicularis muscle suspension. What is proven not to work is simple orbital fat removal. Actually removing orbital fat may even make it look worse by causing a depression above the tear trough which can accentuate it. Thus fat distribution rather than removal is a more effective strategy.
Surgical correction through a lower blepharoplasty can be done using a variety of techniques of which the most effective are orbital fat repositioning and orbicularis muscle suspension. What is proven not to work is simple orbital fat removal. Actually removing orbital fat may even make it look worse by causing a depression above the tear trough which can accentuate it. Thus fat distribution rather than removal is a more effective strategy.
Lower eyelid fat transposition has become the surgical method for treating tear trough deformities. In this technique the orbicularis muscle and septum are separated below the arcus marginalis. This creates an infraorbital depression into which orbital fat is used to fill it. The orbicularis muscle is then suspended out at the lateral canthal area as a preventative manuever to lower the risk of lower eyelid ectropion. (pull down of the lid)
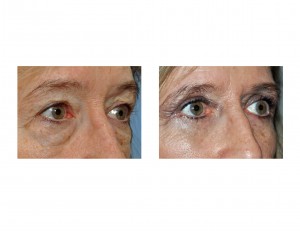
The tear trough deformity is a bothersome aging problem around the eyes that makes one look tired due to their dark circle effect. Injectable fillers are a good first treatment approach and one should stay with the hyaluronic acid-based fillers for these injections. If unsatisfactory results occur then a lower blepharoplasty with fat transposition would be the definitive approach.
Dr. Barry Eppley
Indianapolis, Indiana