

Fractures of the facial bones has occurred since the beginning of time. While the mechanisms of the injury are highly variable and the force needed to break the bone(s) is usually significant, the pattern of the facial bone injury often occurs along predictable and well known fracture lines.
Such is the case with many midface fractures. This is a collection of fracture patterns from nasal, cheek bone , orbital floor and the upper jaw. Upper jaw or maxillary fractures are unique because these midface bones are significantly hollow as they are comprised of air spaces inside the pyriform apertures centrally and the maxillary sinuses laterally. The fracture patterns have been well studied by the French surgeon LeFort and have become known as Left I,II, III fracture patterns based on how the bones break when exposed to a frontal force. This midface fracture classification system is a bit simplistic, and few fractures occur exclusively along the described fracture lines, but it remains useful.
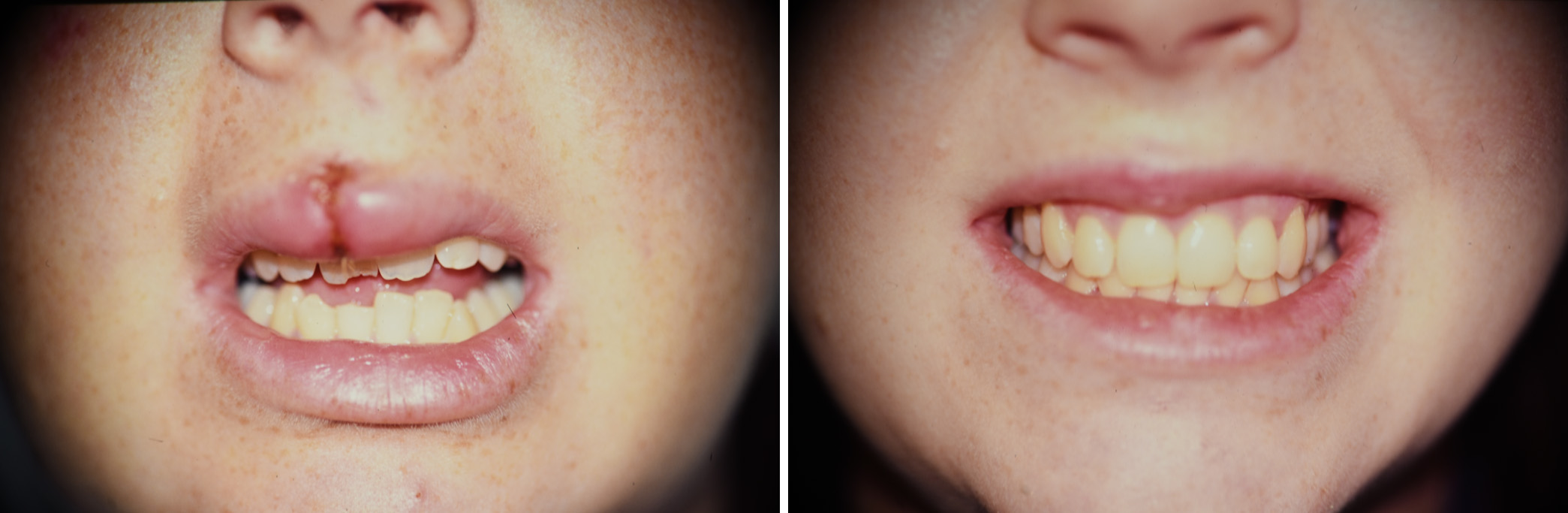
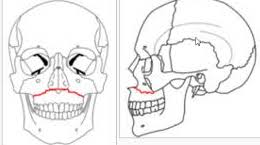 The LeFort I fracture is a horizontal fracture line immediately above the teeth and palate. It takes a frontal force right at the level of the base of the nose and upper lip to create the fracture. They were much more common before the widespread use of seat belts from motor vehicle accidents. While less common today that still do occur and are most manifest by the creation of an intraoral malocclusion, a traumatic class III malocclusion.
The LeFort I fracture is a horizontal fracture line immediately above the teeth and palate. It takes a frontal force right at the level of the base of the nose and upper lip to create the fracture. They were much more common before the widespread use of seat belts from motor vehicle accidents. While less common today that still do occur and are most manifest by the creation of an intraoral malocclusion, a traumatic class III malocclusion.
Surgical treatment of Lefort I fractures consist of open reduction and internal fixation with meal plates and screws after the proper occlusion has been re-established, often with interdental arch bars and wires. The metal plates and screws are placed vertically along the anterior and posterior maxillary buttresses where the bones the thickest. Such metal hardware may or may not cause future issues that require their removal.

 In select Lefort I fractures the metal hardware can be replaced by the use of resorebable plates and screws. (Lactosorb fixation systems) These devices are more technically sensitive than metal devices because of the thinner bone over much of the maxilla except at the buttresses and their need for tapping of the screw holes prior to screw placement. One Lactosorb fixation option to use vertically or obliquely oriented 2.0mm plates and screws.
In select Lefort I fractures the metal hardware can be replaced by the use of resorebable plates and screws. (Lactosorb fixation systems) These devices are more technically sensitive than metal devices because of the thinner bone over much of the maxilla except at the buttresses and their need for tapping of the screw holes prior to screw placement. One Lactosorb fixation option to use vertically or obliquely oriented 2.0mm plates and screws.
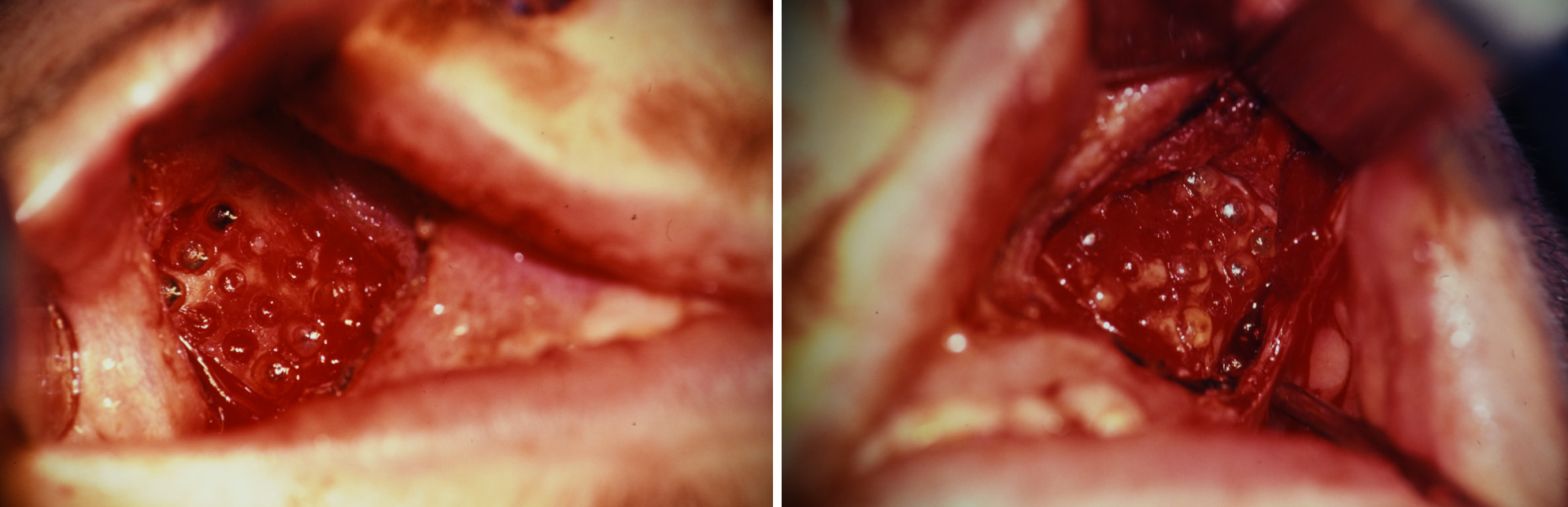
 Another Lactosorb fixation option is to use larger 2.0mm mesh plates which provide complete coverage of the exposed maxillary sinuses. They provide stronger support to the fixation because of the greater amount of material and bone coverage.
Another Lactosorb fixation option is to use larger 2.0mm mesh plates which provide complete coverage of the exposed maxillary sinuses. They provide stronger support to the fixation because of the greater amount of material and bone coverage.
The key to successful use of resorbable fixation in LeFort I fractures is that the occlusion must be set into the preoperative interdigitation state, usually a Class I occlusion. The arch bards are kept in placed through the recovery period should the need arise for any occlusal adjustment or instability.
Dr. Barry Eppley
Indianapolis, Indiana