

Nipples are as variable as the size and shape of breasts. No two nipples are ever exactly alike, usually not even on the same person. While much breast reshaping (breast augmentation, breast reduction, breast lift) goes on in plastic surgery, many men and women suffer from nipple deformities as well which also affects their self-esteem. Nipples can stick out too much, can be turned in, or the areola (the colored area surrounding the nipple) can be too large. Some of these nipple problems may affect certain breast functions such as feeling or lactation. The good news is that there are some very simple plastic surgery procedures that are quite effective at improving these problems.
For the sake of clarification, what most call the nipple is actually two different structures. The true nipple is the central projecting skin area that has both enhanced sensation and milk ducts for lactation. The flatter, almost always more pigmented, skin around the true nipple is called the areola.
Nipple inversion (shy nipple) affects about 2% of the population, more commonly in women than men. Some nipples can be turned in slightly or to a significant degree. Some people are born with nipple inversion, others occur later often after breastfeeding. In rare instances, a tumor may be pulling the nipple inward and this should be ruled out particularly if it occurs later in life and just on one breast. Correction involves a simple procedure done under local anesthesia. The nipple is released and brought out. The biggest problem with nipple inversion correction is relapse, the nipple losing projection and returning to an inward position. Nipple inversion surgery can also be done at the time of other breast surgery. I usually like to delay repair in the case of breast augmentation until later as the implant may help to push out some nipples, making correction unnecessary.
Enlarged nipples often create visible ‘headlights’ which can be a source of embarrassment for many women. This can also be an issue for some men. An overly projecting nipple can be easily reduced through a wedge excision or a ‘ring’ reduction approach. Sensation and the ability for milk production can be preserved with either technique. Done under local anesthesia, nipple reductions are very stable and are not associated with any significant relapse.
“Puffy” nipples can occur in women and are usually associated with the tubular breast deformity. In this nipple problem, the areola and the nipple are pushed outward due to an underlying herniation or protrusion of breast tissue. Correction of this problem is slightly more complex than isolated nipple surgery. It is usually treated as part of tubular breast surgery which involves the use of a breast implant and areolar manipulation. This is treated by making an incision around the areola, removing some of the pigmented skin (if needed), and lifting the areola skin up and decreasing the projection (puffiness). This is a more extensive surgery and requires an operative room experience under anesthesia.
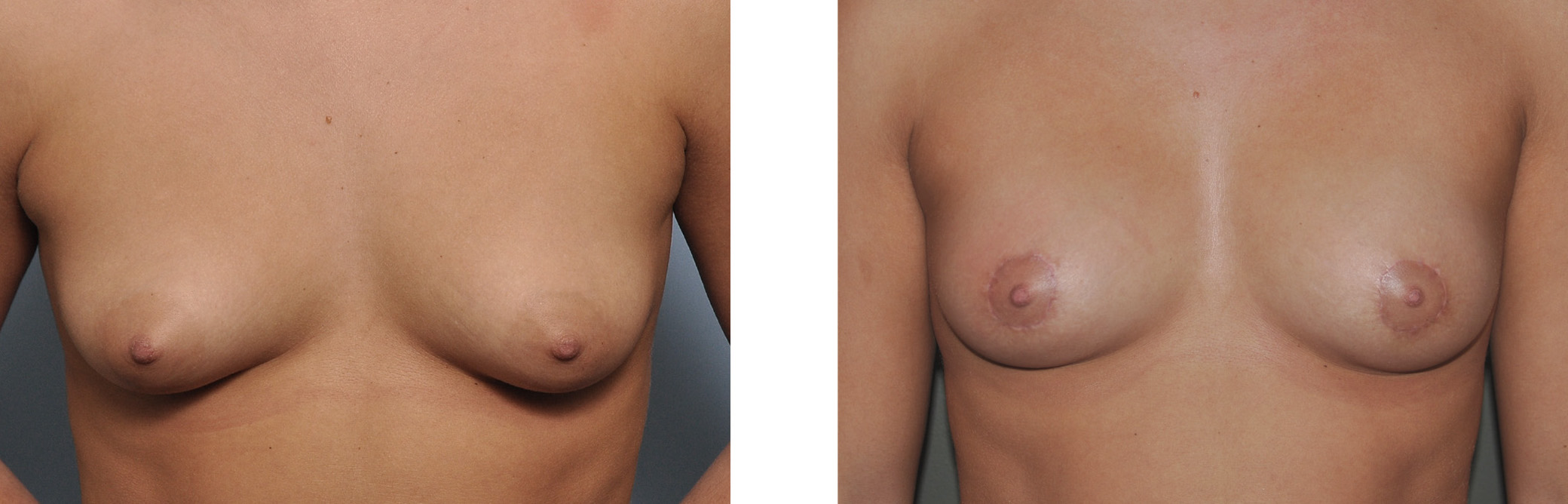 Large or wide areolas are extremely common in big breasts. Usually the size of the areola is related to the size of the breast, but not always. Large areolas are commonly reduced as part of breast reduction surgery. They can be reduced independent of a breast reduction through the periareolar approach. By removing a ring of the outer areola, the circular diameter of the areola is narrowed. Due the tightness of breast skin, there is a limit as to how much the areola can be reduced. This procedure results in a scar at the junction of the areola and skin which occasionally widens and requires secondary revisional surgery.
Large or wide areolas are extremely common in big breasts. Usually the size of the areola is related to the size of the breast, but not always. Large areolas are commonly reduced as part of breast reduction surgery. They can be reduced independent of a breast reduction through the periareolar approach. By removing a ring of the outer areola, the circular diameter of the areola is narrowed. Due the tightness of breast skin, there is a limit as to how much the areola can be reduced. This procedure results in a scar at the junction of the areola and skin which occasionally widens and requires secondary revisional surgery.
Dr. Barry Eppley
Indianapolis, Indiana