

Calf implants involve dissection from incisions on the back of the knee inferiorly down to the gastrocnemius muscle fascia. The fascia is then entered so that the implant can be placed underneath it on top of the muscle.
There are two gastrocnemius muscles, an inner or medial muscle belly and an outer or lateral muscle belly. This requires two separate skin incisions placed above each muscle in the back of the knee in the popliteal skin creases. There is a some distance between the skin incision and the top portion of the muscle which has to be dissected through to reach the fascia.
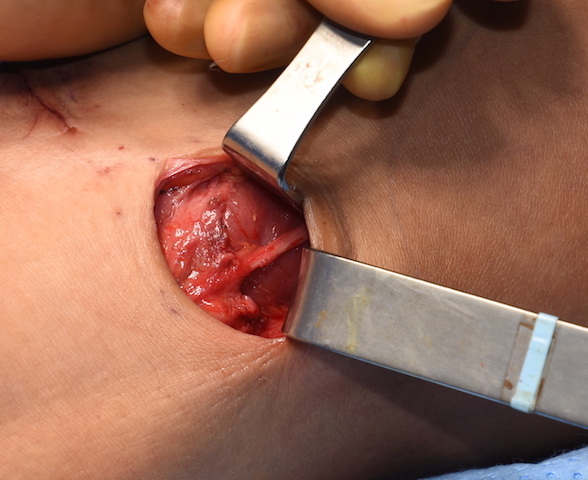
 Once making the incision and along the course of this dissection it is common to see nerve branches. These superficial nerves are typically small in size and are cutaneous branches of the sural nerve which supplies sensation to various skin regions of the back of the leg. But during the dissection down to the lateral muscle head a much larger nerve may occasionally be seen which should not be confused with a cutaneous nerve branch.
Once making the incision and along the course of this dissection it is common to see nerve branches. These superficial nerves are typically small in size and are cutaneous branches of the sural nerve which supplies sensation to various skin regions of the back of the leg. But during the dissection down to the lateral muscle head a much larger nerve may occasionally be seen which should not be confused with a cutaneous nerve branch.
The common peroneal nerve (also called the common fibular nerve) is the terminal branch of the sciatic nerve which courses along the upper lateral side of the popliteal fossa and is usually located along the medial border of the biceps femoris muscle, most typically deep to the muscle on its way to the fibular head. This larger nerve will occasionally be seen when its course is more superficial than deep during placement of a lateral calf implant. When more superficial the nerve runs right between the biceps femoris muscle fascia and the most lateral aspect of the lateral gastrocnemius fascia. As a result it is potentially exposed to being traumatized by the course of the dissection or the retraction needed to place the implant.
Injury to this common peroneal nerve can result in foot drop in which the foot can not dorsiflex and the foot drags during walking. It can also result in loss of sensation to the dorsal surface of the foot. If such a nerve injury occurs it will be evident immediately after surgery.
I have only seen the common peroneal nerve a few times during placement of lateral calf implants and have had two patients with short and longer term foot drops as a result. While it is a motor nerve that can recover it can be a long process. As a result I now advise my patients that of I see the common peroneal nerve during the dissection I will not go forward and place the implant. It is not worth the potential risk of even a short term nerve injury. Also the medial calf implant is always the most aesthetically important one so a risk of nerve injury is not worth it for the less significant cal muscle augmentation.
Dr. Barry Eppley
Indianapolis, Indiana