

While cheek implants are of the most commonly performed synthetic facial augmentation procedures, they are unique in several ways. One of their unique features is that they are typically placed in an upward direction from below (intraoral) and are positioned essentially ‘on the side of a clift’ so to speak. Laying up against the prominence of the cheek bone (body of the zygoma) they are on a surface that is not flat but has a rather steep angle.
As a result of placing cheek implants at a bit of an angle, and the need to have a subperiosteal tissue pocket that is bigger than the implant (a necessity to ensure all edges of the implant are laying flat), the intraoperative question arises as to whether the implant will stay were placed. Or once the incision is closed what assurance does one have that the cheek implant won’t move?
This potential concern has led to an often back and forth debate about the need for some form of fixation of the implant. Some surgeons argue that it is not necessary and feel confident their pocket creation and implant placement is adequate. Other surgeons employ fixation techniques that range anywhere from external bolsters, internal suturing to screw fixation.
In the end it is what the surgeon feels comfortable doing and what their experiences has shown that works. I almost always employ screw fixation and have done so for years with most cheek implants. One key in its use is the development of the auto-drive screw that does not need a drill. They are simple to use and go in easy into the softer bones of the midface.
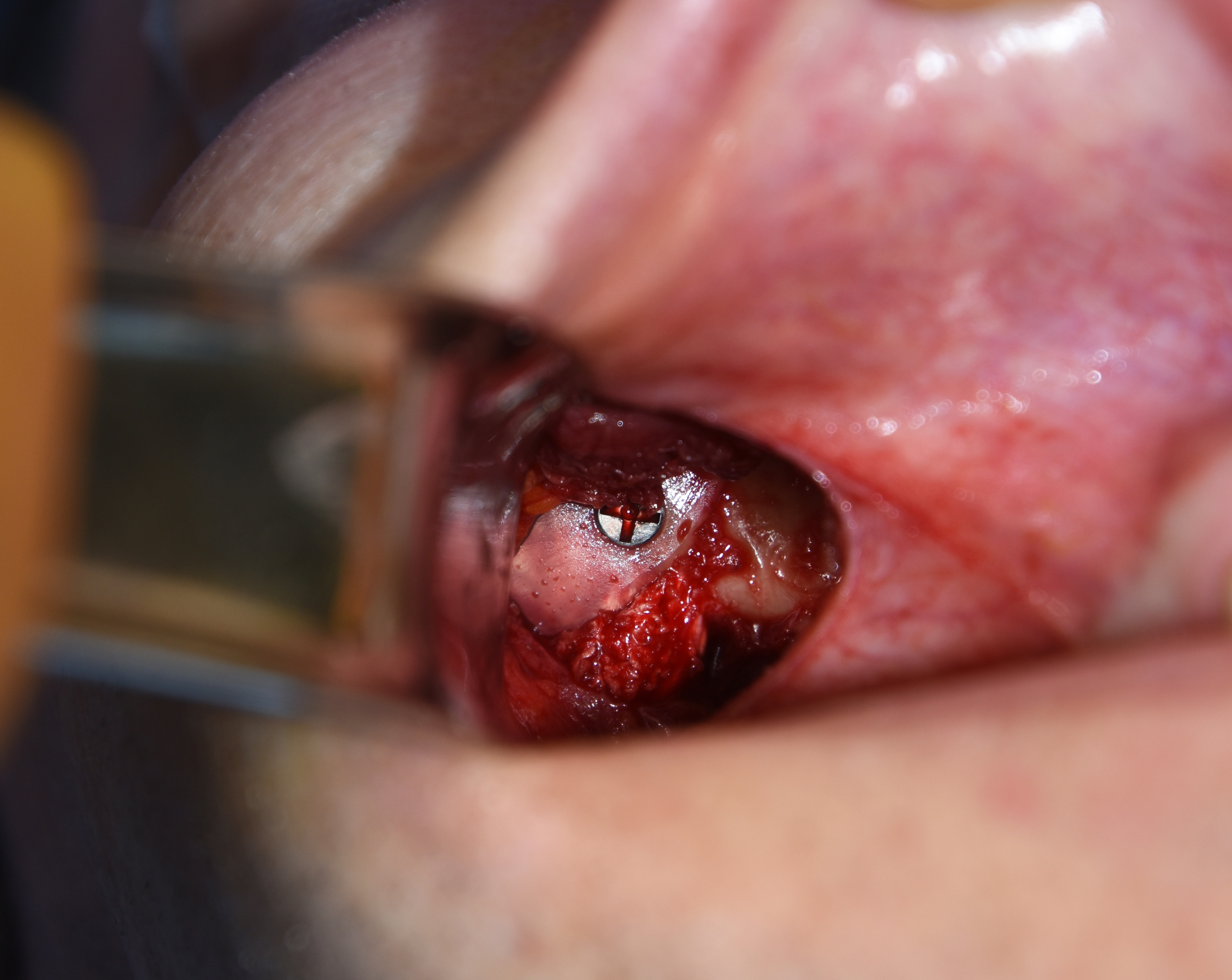 But one key to avoid with their use is to put them into the maxillary bone right over the maxillary sinus. With a screw tip sticking into the sinus cavity this is a potential source of sinus bacteria tracking along the screw out onto the implant and causing an infection. To avoid this adverse scenario I advise placing the screw into solid cortical bone at the posterior zygomatic buttress or the body of the zygoma itself. This can be a little more technically difficult to do sometimes but is well worth the piece of mind that there is no chance of a sinus communication to the implant site.
But one key to avoid with their use is to put them into the maxillary bone right over the maxillary sinus. With a screw tip sticking into the sinus cavity this is a potential source of sinus bacteria tracking along the screw out onto the implant and causing an infection. To avoid this adverse scenario I advise placing the screw into solid cortical bone at the posterior zygomatic buttress or the body of the zygoma itself. This can be a little more technically difficult to do sometimes but is well worth the piece of mind that there is no chance of a sinus communication to the implant site.
While many surgeons debate the value of screw fixation of cheek implants, almost always due to their unfamiliarity and comfort with their use, it is hard to argue with assured implant positioning with a technique that takes little time and extra expense.
Dr. Barry Eppley
Indianapolis, Indiana