

The sagging or downturned corner of the mouth is not a facial feature that anyone requests to have. While the fall of the corner of the mouth is most commonly associated with aging, due to the weight of the overlying falling softy tissues, some people have a natural downward slant to the corners of their mouth. Such mouth positions convey a non-dynamic expression of sadness or even mad appearance.
The surgical repositioning of the mouth corners has been done for over a hundred years beginning with intraoral techniques to try and elevate them. This evolved to external skin excisional methods with improved results but with visible scarring. The classic ‘Valentine’ method effectively lifts the mouth corners by leaves a scar that trails away from the mouth corners…which would rely be acceptable for most patients.
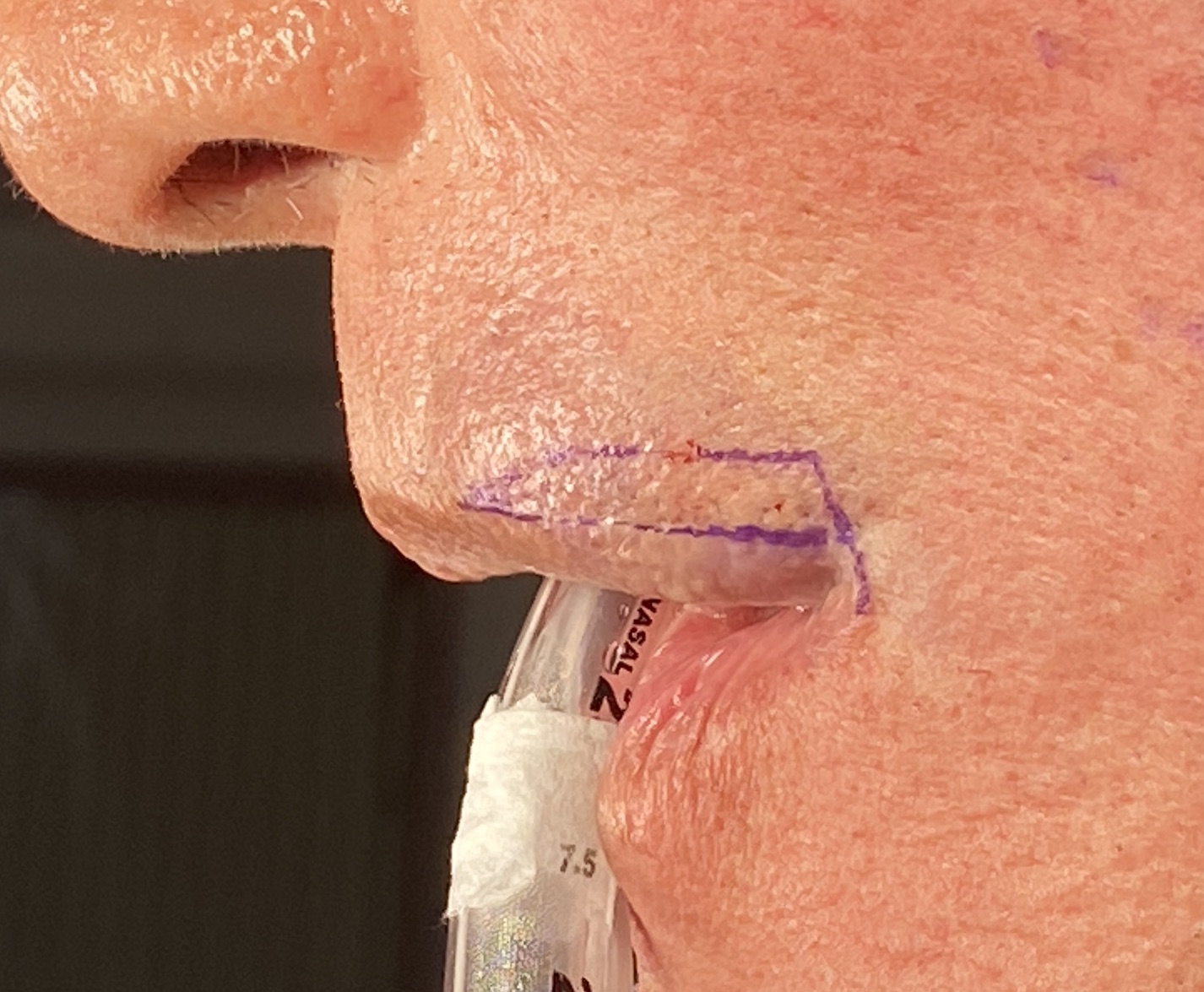
 The pennant technique for a mouth corner lift uses a tissue relocation that moves the flexible vermilion of the joined upper and lower lip into the skin excision site. This keeps the scars line at the vermilion-cutaneous junction. But another important element of the corner lift its how it blends into the rest of the upper lip. If the horizontal limb of the pennant marking is too short the mouth corner can have a visible angulation upward or a curl. This is actually how corner curls are made but most do not want that look. As a result the horizontal limb of the pennant excision must be longer so that the outer upper lip blends into mouth corner in a smooth fashion along the vermilion-cutaneous edge.
The pennant technique for a mouth corner lift uses a tissue relocation that moves the flexible vermilion of the joined upper and lower lip into the skin excision site. This keeps the scars line at the vermilion-cutaneous junction. But another important element of the corner lift its how it blends into the rest of the upper lip. If the horizontal limb of the pennant marking is too short the mouth corner can have a visible angulation upward or a curl. This is actually how corner curls are made but most do not want that look. As a result the horizontal limb of the pennant excision must be longer so that the outer upper lip blends into mouth corner in a smooth fashion along the vermilion-cutaneous edge.
 The extended pennant excision technique creates a smoother fuller upper lip appearance at its lateral aspect that blends into the uplifted corner. Before the transposed vermilion corner is lifted upward into the excision site a wedge of orbicularis muscle is removed to give it an unobstructed repositioning. Such muscle removal may also prevent some of the downward pull on the uplifted corner.
The extended pennant excision technique creates a smoother fuller upper lip appearance at its lateral aspect that blends into the uplifted corner. Before the transposed vermilion corner is lifted upward into the excision site a wedge of orbicularis muscle is removed to give it an unobstructed repositioning. Such muscle removal may also prevent some of the downward pull on the uplifted corner.
Dr. Barry Eppley
World-Renowned Plastic Surgeon