

Background: The natural temporal shape for most people is either a flat profile or a slight concavity. This shape is defined by a line drawn between the bony temporal line of the forehead superiorly and the zygomatic arch bone inferiorly. It may touch it (flat profile) or have a 1mm space beneath it. (slight concavity) While there may be patients that prefer a convex shape or even a more pronounced concavity, the aesthetic norm appears to be a flat or slightly concave shape.
One common sequelae of aging, which often is more pronounced in females, is the development of an excessive temporal concave shape or hollowing. The hollowing is usually due to the loss of fat in the temporal muscle rather than loss of muscle mass itself. Temporal hollowing is defined by a skeletonized or sunken appearance to the temporal region revealing the bony borders of the forehead (temporal line) and the lateral orbital rim.
Temporal hollowing can be treated by either non-surgical (synthetic fillers), minimal surgical (fat injections) and surgical. (implants) Each method has their advantages and disadvantages but for an assured permanent effect temporal implants provide that effect. Today’s temporal implants are placed through small incisions in the hair bearing area and are placed on top of the muscle but under the fascia. Historically attempts at temporal implants failed because they were placed in the subcutaneous level where their outlines will eventually be seen. Implants or bone cements can be placed underneath the muscle in the deep temporal fossa bone but it takes a lot of volume to create an external effect and control of the external shape is less predictable. For aesthetic temporal augmentation the subfascial location is ideal….straightforward surgery and predictable effect.
The choices in temporal implants are whether to use standard or custom implants as well as what thickness should they be. Custom implants may be used in very severe hollowing, if significant asymmetry is present or the implant coverage (footprint) is needed beyond what the standard implant can provide. For implant thickness there is no exact science to it and no exact method by which to measure and determine it. The key is to avoid an unnatural appearance (over correction) or too much convexity.
Case Study: This female developed significant temporal hollowing which was greater on her left side than the right. Custom temporal implants were designed and placed and she recovered uneventfully. When judging the result three months after surgery she felt the left temporal region had too much convexity and the right only slightly so.
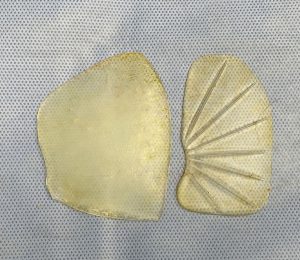
 Under general anesthesia the custom temporal implants were removed and replaced with 3mm standard temporal implants through her very small existing incisions.
Under general anesthesia the custom temporal implants were removed and replaced with 3mm standard temporal implants through her very small existing incisions.


 Her intraoperative before and after pictures showed the slight but significant change in the temporal shape with a slight concavity.
Her intraoperative before and after pictures showed the slight but significant change in the temporal shape with a slight concavity.
Having done many temporal implants when it comes to the need for secondary revisions it is due to either too much convexity or the implant isn’t up tight against the  lateral orbital wall and bony temporal line. When it comes to convexity vs a concavity a millimeter or two can make all the difference. No matter how severe the temporal hollowing is it is best to provide a correction that still maintains some slight hollowing to it.
lateral orbital wall and bony temporal line. When it comes to convexity vs a concavity a millimeter or two can make all the difference. No matter how severe the temporal hollowing is it is best to provide a correction that still maintains some slight hollowing to it.
Case Highlights:
1) The definitive and permanent treatment for temporal hollowing are implants placed in top of the muscle in the subfascial plane.
2) In significant temporal hollowing that is asymmetric custom temporal implants are a logical choice.
3) In females the difference between a pleasing temporal shape and too much convexity can be as small as one millimeter.
Dr. Barry Eppley
Indianapolis, Indiana