

Facial reshaping is both a patient’s aesthetic goal as well as a surgical strategy. Patient goals are often stated, as an example, of desiring slimmer or more defined facial features. Patients may have some idea as to what procedures may help achieve that effect but may not know all their options nor how they work to achieve a collective facial change.
Most facial reshaping surgeries are often a collection of reductive and augmentative procedures that done together are more successful than any go the procedures done alone. This is a surgical strategy known as diametric facial reshaping. It has an established historical precedent in the well known combination of a reduction rhinoplasty and a chin augmentation. This is the most basic type of diametric facial reshaping surgery which is easiest to understand because it is mainly a profile facial change.
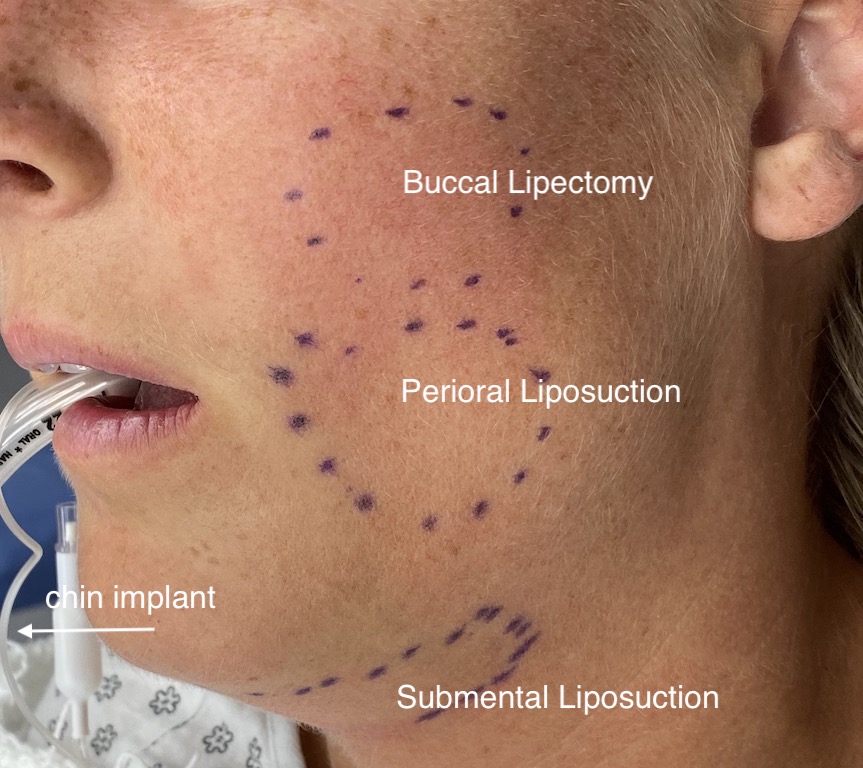
 But there are many other examples in facial reshaping surgery whose effects may be better appreciated in the frontal or oblique views. In my experience one of these common types of diametric facial reshaping is based on fat reduction and bony chin augmentation. The main facial and neck harvest sites from the buccal fat pads (buccal lipectomy), lower cheeks/jowls (perioral/jowl microliposuction and neck (submental liposuction) are combined with a chin augmentation. (implant or sliding genioplasty)
But there are many other examples in facial reshaping surgery whose effects may be better appreciated in the frontal or oblique views. In my experience one of these common types of diametric facial reshaping is based on fat reduction and bony chin augmentation. The main facial and neck harvest sites from the buccal fat pads (buccal lipectomy), lower cheeks/jowls (perioral/jowl microliposuction and neck (submental liposuction) are combined with a chin augmentation. (implant or sliding genioplasty)
The goal of this type of diametric facial reshaping is to draw in the soft tissues that surround the projections of the chin and cheek to end up with a less round/more defined face. This is a combined soft tissue-bone change that differs from the rhinoplasty-chin augmentation which uses hard tissue on both the augmentation and reduction sides of the change.
There are numerous other examples of the strategy of diametric facial reshaping. But the key takeaway is that multiple changes going in different directions always creates the most significant facial shape changes.
Dr. Barry Eppley
Indianapolis, Indiana