

 While numerous types of implants exist for many areas of the face, the central midface has only ever had one implant style. The well known although infrequently used Peri-Pyriform implant, as the name indicates, provides an augmentation around the base of the nose. This anatomically is known as the pyriform aperture which serves as the bony entrance to the nasal cavity and hence the name of the implant.
While numerous types of implants exist for many areas of the face, the central midface has only ever had one implant style. The well known although infrequently used Peri-Pyriform implant, as the name indicates, provides an augmentation around the base of the nose. This anatomically is known as the pyriform aperture which serves as the bony entrance to the nasal cavity and hence the name of the implant.
Technically and of importance when determining nasal base augmentation needs is that the pyriform aperture area is divided into two distinct augmentation zones. The paranasal area is on the side of the pyriform aperture and includes the canine fossa and the maxilla lateral to it. I prefer to call this the paranasal-maxillary augmentation zone. The central pyriform aperture is the premaxillary augmentation zone which includes the anterior nasal spine under the base of the columella and the area above the central and lateral incisor teeth. Thus in evaluating central midface augmentation needs one has to determine if the augmentation should include just one or both of these central midface augmentation zones.
The existing preformed peri-pyriform implant, while sounding inclusive, has a deficient design. Like many such implants that have been advocated in the medical literature for the area they have a history of being done in conjunction with rhinoplasty and were designed to really be a soft tissue implant placed from an intranasal incision. Besides not being in a subperiosteal location, which can cause issues with smiling and upper lip movement, it is a rounded edge implant. This results in a very palpable feel to the implant which is a reflection of both its rounded edges and inadequate extension further out onto the maxilla. When you combine a very round edge and the natural depression from the canine fossa at its sides it will both look and feel like an ‘implant’.
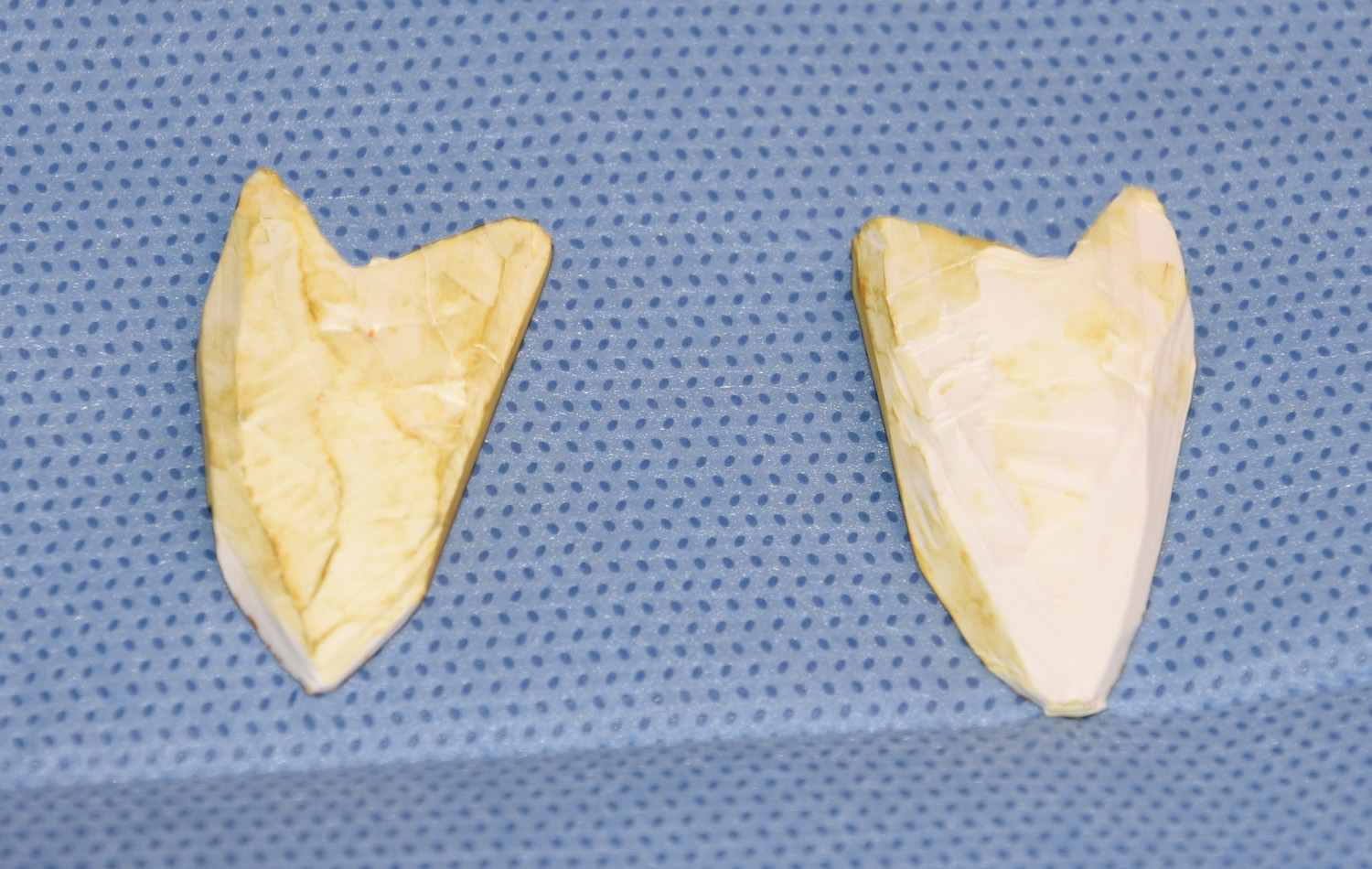
 Until a better premaxillary-paranasal-maxillary implant design becomes available as an off-the-shelf product, I prefer to make my own implant intraoperatively. Using a 5mmm to 7mm thick ePTFE block, the paranasal-maxillary implant is fashioned to provide fullness right up under the base of the nostrils but with an extension that covers the canine fossa in a tapering fashion out laterally. This provides better paranasal augmentation that looks and feels natural. (meaning you can’t feel the implant) This is a subperiosteal implant that is placed through an intraoral incision that will have any detrimental impact on upper lip movement.
Until a better premaxillary-paranasal-maxillary implant design becomes available as an off-the-shelf product, I prefer to make my own implant intraoperatively. Using a 5mmm to 7mm thick ePTFE block, the paranasal-maxillary implant is fashioned to provide fullness right up under the base of the nostrils but with an extension that covers the canine fossa in a tapering fashion out laterally. This provides better paranasal augmentation that looks and feels natural. (meaning you can’t feel the implant) This is a subperiosteal implant that is placed through an intraoral incision that will have any detrimental impact on upper lip movement.
A premaxillary implant can also be hand carved in the same fashion to cover the anterior nasal spine and the inferior pyriform aperture edge. The keys again to a natural implant are a feathering edge design and intraoral placement.
Dr. Barry Eppley
Indianapolis, Indiana