

Custom skull implants are one of the main surgical options used to improve cranial asymmetry in adult plagiocephaly when the skull bones can no longer be reshaped. In adults, the cranial sutures are fused, so correction is typically done by augmenting the skull contour rather than moving bones.
Below is a structured overview of how custom skull implants are used in these cases.
Custom Skull Implants for Adult Plagiocephaly
1. Basic Concept
Adult plagiocephaly correction is usually performed using extracranial augmentation implants placed over the skull to restore symmetry.
- The implant is placed on top of the skull bone under the scalp.
- The skull itself is not cut or repositioned.
- The procedure is primarily aesthetic contour correction rather than cranial vault remodeling.
This makes it significantly less invasive than cranial vault reconstruction used in infants.
2. Implant Design Process
Custom implants are patient-specific and typically designed from 3D CT imaging.
Workflow
- CT scan of the skull
- 3D digital reconstruction
- Mirror-image modeling of the normal side
- Implant design to fill flattened areas
- CAD/CAM or 3D printing fabrication
The result is an implant that precisely matches the patient’s skull anatomy.
3. Implant Materials
Common materials include:
Silicone elastomer
- Most common for aesthetic skull contouring
- Flexible and easy to place
- Feathered edging
PEEK (polyether ether ketone)
- Ultra rigid material
- Used more in skull reconstructions for full thickness defects
Titanium
- Sometimes used in reconstructive cranial implants
- Not appropriate for use as a bone onlay augmentation material
Each material is biocompatible and designed to last indefinitely.
4. Surgical Technique
Typical steps:
- Small scalp incision
- Subperiosteal pocket created
- Implant inserted and positioned
- Fixation with small titanium screws
- Scalp closure
Implants become stable through primary screw fixation and secondary tissue encapsulation.
5. Areas Treated in Plagiocephaly
Adult plagiocephaly often requires correction of:
Most common
- Unilateral occipital flattening (back of the head)
Sometimes also
- Contralateral forehead flattening
- Temporal hollowing
- Parietal asymmetry
In more complex cases, multiple implants (forehead + occiput) may be used in one surgery.
6. Limitations
Custom implants improve contour but do not correct underlying cranial rotation.
What can be corrected:
- Flat areas
- Skull contour asymmetry
- Visible head shape imbalance
What usually cannot be corrected:
- Ear position asymmetry
- Orbital skeletal rotation
- Facial asymmetry related to cranial torsion
7. Risks and Complications
Overall complication rates are relatively low but include:
- Infection
- Seroma/hematoma
- Implant visibility or palpability
- Need for revision
- Rare implant removal
General cranioplasty literature reports infection risks around 1-2% depending on materials and case complexity.
8. Outcomes
Most patients undergo surgery for cosmetic improvement and psychological benefit.
Studies of custom cranial implants show:
- High accuracy of fit
- Good aesthetic outcomes
- Long-term implant durability
Key Point:
Adult plagiocephaly correction with custom implants is essentially a skull contour augmentation procedure, not a cranial reconstruction.
Case Study
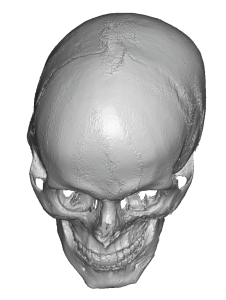
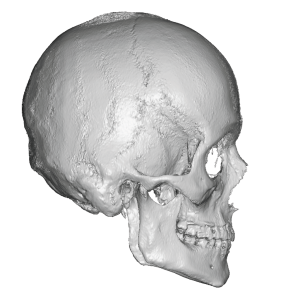
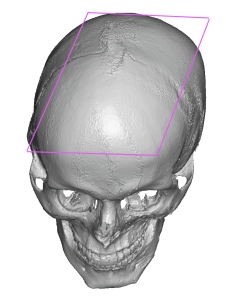 This male had congenital plagiocephaly with clockwise rotation of skull and face (the most rotation seen) with a right occipital-temporal flattening, left occipital temporal protrusions and some left facial retrusions. The posterior skull was more severely affected than that of the face. It had the classic parallelogram deformity.
This male had congenital plagiocephaly with clockwise rotation of skull and face (the most rotation seen) with a right occipital-temporal flattening, left occipital temporal protrusions and some left facial retrusions. The posterior skull was more severely affected than that of the face. It had the classic parallelogram deformity.
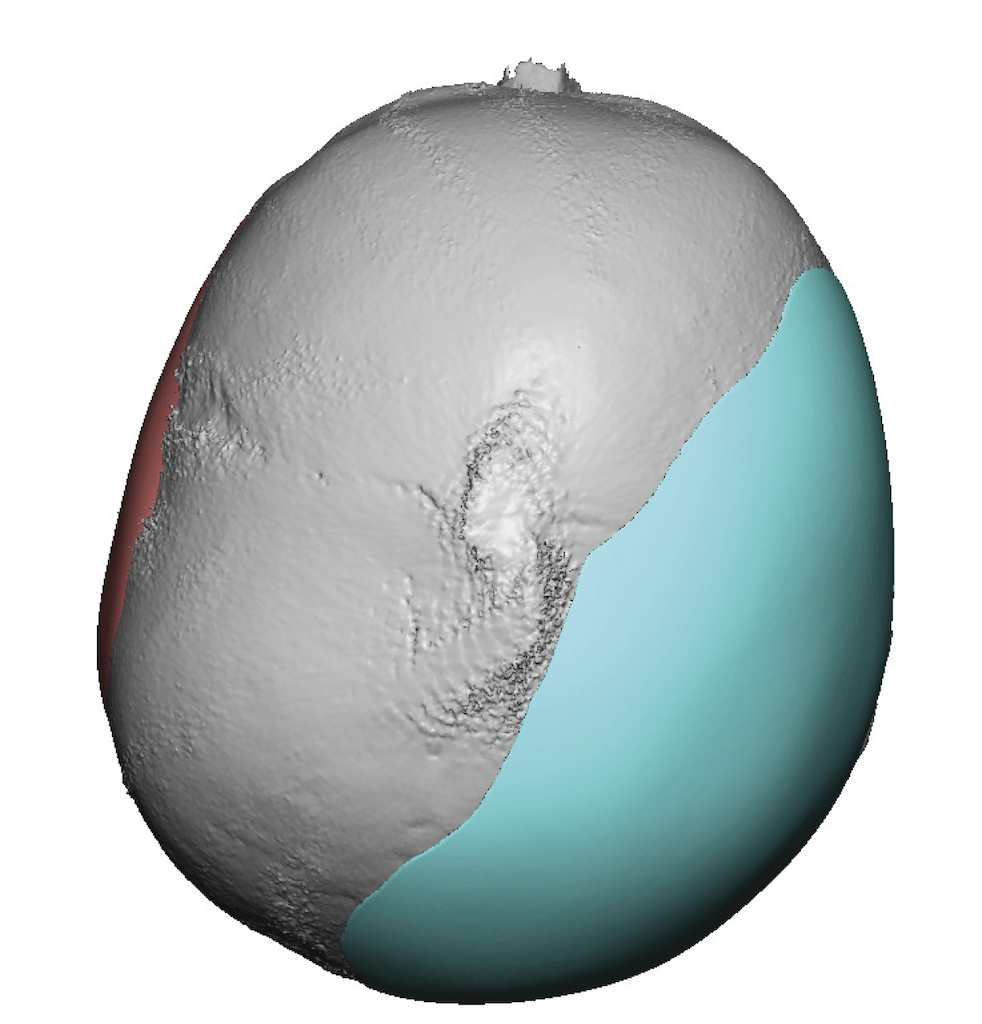
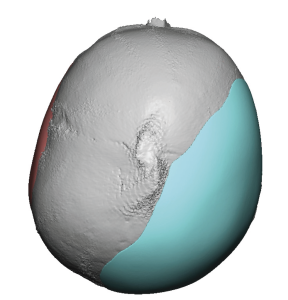 The plan for correction was right custom skull augmentation, left temporal-parietal reductions and left midface and jawline augmentation. The custom skull implant was designed to augment the flattened right side of the flat back of the head. It did not need to stick out as far as the protrusive left side.
The plan for correction was right custom skull augmentation, left temporal-parietal reductions and left midface and jawline augmentation. The custom skull implant was designed to augment the flattened right side of the flat back of the head. It did not need to stick out as far as the protrusive left side.
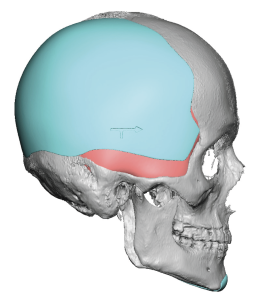 To accurately correct the right sided flatness it needed to extend way forward to the anterior temporal area.
To accurately correct the right sided flatness it needed to extend way forward to the anterior temporal area.
There were also left sided facial implants designed but this is not pertinent to this skull implant case study.

 The large right custom skull implant was placed through an existing hair transplant scar on the back of his head aided by two smaller anterior incisions to help with pocket dissection and for screw fixation.
The large right custom skull implant was placed through an existing hair transplant scar on the back of his head aided by two smaller anterior incisions to help with pocket dissection and for screw fixation.
This implant produced a significant improvement and two years later a smaller right custom skull implant overlay was added to optimize the correction of the right skull flatness.

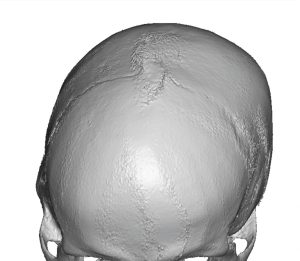
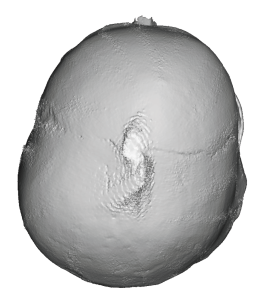
 His result showed the skull shape improvement with improved symmetry. It is still a larger head but one with now better shape.
His result showed the skull shape improvement with improved symmetry. It is still a larger head but one with now better shape.
Discussion
 Rotational plagiocephaly (also called deformational cranial torsion) is the most common pattern of adult skull asymmetry treated with custom implants. The key challenge is that the skull is not simply flat on one side—the entire cranial vault is rotated along a diagonal axis, creating a parallelogram shape.
Rotational plagiocephaly (also called deformational cranial torsion) is the most common pattern of adult skull asymmetry treated with custom implants. The key challenge is that the skull is not simply flat on one side—the entire cranial vault is rotated along a diagonal axis, creating a parallelogram shape.
Because implants add volume but cannot move bone, implant design must strategically camouflage the rotational deformity.
Below are the main implant design strategies used for adult rotational plagiocephaly correction.
1. Mirror-Image Modeling (Baseline Strategy)
Concept
Use the normal side of the skull as a template.
Process
- Generate a 3D CT skull model
- Mirror the normal posterior skull
- Overlay it onto the flattened side
- Design implant to fill the missing projection
Best for
- Mild–moderate unilateral occipital flattening
Limitation
Pure mirror correction can over-widen the skull if rotational asymmetry is significant.
2. Diagonal Augmentation Strategy
Rotational plagiocephaly produces asymmetry along a diagonal axis:
Typical pattern:
- Flat occiput (one side)
- Contralateral parietal bossing
- Ipsilateral forehead flattening
- Contralateral forehead prominence
Implant design principle
Augment only the deficient diagonal.
Example pattern:
|
Region |
Treatment |
|
Flat occiput |
Major augmentation |
|
Ipsilateral parietal |
Moderate augmentation |
|
Contralateral parietal bossing |
No augmentation |
|
Ipsilateral forehead |
Optional implant |
Goal: restore diagonal symmetry without exaggerating width.
3. Posterior Skull Expansion Strategy
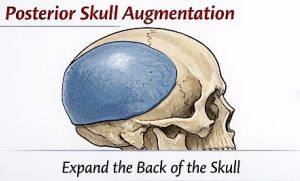 This is the most common adult correction.
This is the most common adult correction.
Design focus
Occipital augmentation extending into:
- Posterolateral parietal bone
- Mastoid region
- Upper nuchal region
Implant characteristics
Typical thickness:
- 5–15 mm central augmentation
Typical volume:
- 25–80 cc
Design rule
Implants should feather out gradually across:
- lambdoid region
- superior parietal vault
This prevents a visible implant edge.
4. Counter-Rotation Camouflage
True rotational deformity cannot be corrected surgically without cranial osteotomies. Instead, implant design creates visual counter-rotation.
Method
Augment areas that visually reverse the rotation.
Example:
Original rotation pattern:
Left occiput flat
Right parietal prominent
Left forehead flat
Right forehead prominent
Camouflage correction:
- Left occipital implant
- Left parietal augmentation
- Left forehead implant (optional)
This visually rebalances the cranial axis.
5. Dual-Implant Strategy
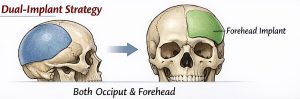 Moderate–severe plagiocephaly often requires two implants.
Moderate–severe plagiocephaly often requires two implants.
Common combinations
Posterior implant
- Occipital flattening correction
Anterior implant
- Forehead flattening correction
Benefits:
- Restores cranial diagonal balance
- Improves profile symmetry
Typical volumes:
- Occipital: 40–90 cc
- Forehead: 5–25 cc
6. Parietal Width Control
One major design pitfall is creating excessive skull width.
Key rule:
Never fully mirror the opposite side in severe plagiocephaly.
Instead use:
- partial mirror modeling
- smooth interpolation curves
Goal:
Maintain natural cranial width.
7. Edge Blending and Implant Feathering
Implants must taper gradually across the skull surface.
Typical feather zones:
- Parietal vault
- Temporal line
- Occipitomastoid junction
Thickness transition often reduces from:
- 10–12 mm centrally
- to 0 mm over 3–5 cm
This avoids:
- palpable edges
- visible step-offs.
8. Scalp Stretch Limit Consideration
The scalp limits implant size.
General safe limits:
|
Region |
Typical max thickness |
|
Occipital |
15–18 mm |
|
Parietal |
10–12 mm |
|
Forehead |
6–8 mm |
Larger corrections may require:
- staged expansion
- smaller compromise implant.
9. Symmetry Metrics Used in Design
Modern CAD planning evaluates:
- Cranial vault asymmetry index (CVAI)
- Diagonal difference
- Posterior cranial vault symmetry
- Skull width ratios
These help quantify improvement before surgery.
10. Incision-Driven Implant Design
Implant geometry must also match surgical access.
Common incisions:
- posterior scalp incision
- occipital hairline incision
- bicoronal (for combined forehead correction)
Implants are sometimes segmented so they can pass through smaller incisions.
Key Design Principle
The goal is visual symmetry rather than geometric symmetry.
Perfect mirroring often produces:
- overly wide skull
- unnatural contours
Good design prioritizes:
- natural cranial curvature
- balanced diagonal projection
- smooth contour transitions.
? In summary
Effective implant correction of rotational plagiocephaly typically involves:
- Posterior skull augmentation
- Diagonal contour balancing
- Selective parietal expansion
- Optional forehead implant
rather than simple mirror-image filling.
Dr Barry Eppley
Plastic Surgeon