

Background: Cheek implants can have variable locations of placement over the cheek or zygomatic bone. But in many cases the placement of cheek implants will have their anterior or inferior located onto portions of the maxilla. Many times this is onto the thicker bone of the posterior maxillary buttresses and less frequently onto the thinner bone of the maxillary sinus wall. This occurs due to either their desired placement location or as a result of the intraoral incisional access. (unintentional placement)

 Because of potential maxillary involvement and the not uncommon biologic sequelae of implant settling there is always the risk of maxillary sinus exposure when cheek implants are removed and replaced. Since it is never a good idea to place an implant over or around an opening into the maxillary sinus it is important to be aware of this potential before surgery and to be prepared for what to do should it be encountered.
Because of potential maxillary involvement and the not uncommon biologic sequelae of implant settling there is always the risk of maxillary sinus exposure when cheek implants are removed and replaced. Since it is never a good idea to place an implant over or around an opening into the maxillary sinus it is important to be aware of this potential before surgery and to be prepared for what to do should it be encountered.
In cheek implant replacements, which in my experience is most commonly done with custom cheek implant designs, it is extremely helpful to know the current implant shape, size and location of both sides. In the 3D CT scan that is needed to design the implants the existing cheek implants can be seen…if they are silicone. The other commonly used facial implant material, Medpor, can not usually be seen in 3D scans. While seen in 2D CT scans the material is not seen in 3D reconstructions. This poses some challenges in the new implant designs.
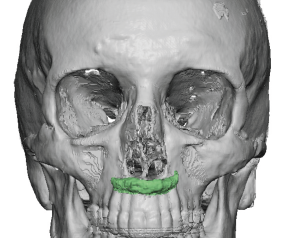
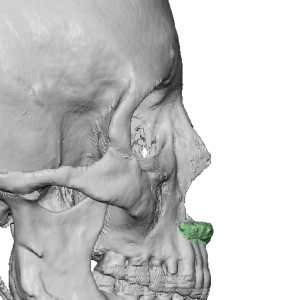 Case Study: This older female had cheek implants placed 25 years ago through an intraoral approach. Their type and size/shape were unknown. A 3D CT scan showed a hint of the implant imprint on the bone indicating it was a Medpor material. There was also the knowledge that decades ago there were only so many Medpor implant possibilities.
Case Study: This older female had cheek implants placed 25 years ago through an intraoral approach. Their type and size/shape were unknown. A 3D CT scan showed a hint of the implant imprint on the bone indicating it was a Medpor material. There was also the knowledge that decades ago there were only so many Medpor implant possibilities.
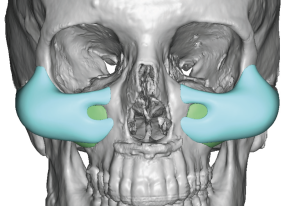
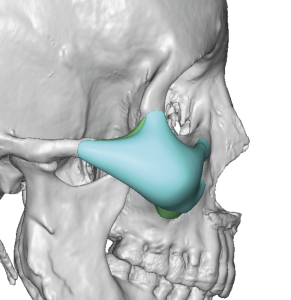 Using her 3D CT scan the imprint of the existing Medpor implants was colored in and made to the level of the surrounding bone. Large custom cheek implants were designed per her request in an effort to increase her existing cheek augmentation effect to the point that it had a significant cheek lifting effect. Their maximum projection was an aggressive 12mm with a combined implant volume of 15ccs.
Using her 3D CT scan the imprint of the existing Medpor implants was colored in and made to the level of the surrounding bone. Large custom cheek implants were designed per her request in an effort to increase her existing cheek augmentation effect to the point that it had a significant cheek lifting effect. Their maximum projection was an aggressive 12mm with a combined implant volume of 15ccs.
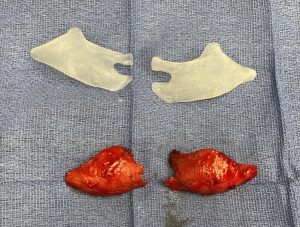



 Under general anesthesia and through her existing intraoral maxillary vestibular scars, the Medpor cheek implants were fairly easily removed since they were mobile due to their very low position on the maxilla. Their convex shape over the concave maxilla allowed for limited implant-bone contact. Once removed they were replaced with the larger custom cheek implants with single screw fixation per side.
Under general anesthesia and through her existing intraoral maxillary vestibular scars, the Medpor cheek implants were fairly easily removed since they were mobile due to their very low position on the maxilla. Their convex shape over the concave maxilla allowed for limited implant-bone contact. Once removed they were replaced with the larger custom cheek implants with single screw fixation per side.
Case Highlights:
1) Medpor cheek implants are often not seen on 3D CT scans no matter how long they have been implanted.
2) Before removing Medlor cheek implants, particularly of replacements are to be done, it is important to check preoperatively whether implant settling has caused maxillary sinus exposure.
3) When designing custom cheek implants for replacement of Medpor implants which can’t usually be seen on 3D CT scans, one should be prepared to do intraoperative reduction based on how they look when implanted.
Dr. Barry Eppley
Indianapolis, Indiana