

Background: In the male a strong jawline is a desired facial feature. There are no really defective ways to create a strong jawline other than by surgery. This is particularly true in the male who has a naturally weak or underdeveloped lower jaw. Interestingly jaw muscle exercises have been touted as a method to increase the width of the lower jaw over the posterior angles where the masseter muscles exist. However, while the effectiveness of these exercises can be debated, suffice it to say it would be limited and uncertain as to their long-term maintenance of the muscle hypertrophy.
One of the more common aesthetic lower jaw deformities is that of the high mandibular plane angle jaw shape. This is where the lower jaw is rotated up and backwards, creating a high posterior jaw angle and a short recessive chin. In essence, the L shape of the lower jaw is altered to a decreased horizontal position. Correction of the high mandibular plane angle patient requires derotation of the L shape, vertically lengthening the jaw angles and bringing the chin forward.
How much vertical lengthening of the jaw that is needed requires assessment of the gonial angle that exists compared to the type of angle the patient wants. As a general rule, a gonial angle that exceeds 140° would be considered aesthetically deficient while a gonial angle less than 110° would be considered aesthetically too prominent. Within the wide range of 110 to 140° for the gonial angle leaves a lot of room for patient preference. Choosing the best gonial angle for any particular patient must factor in other facial features as well. There is no perfect gonial angle that would apply to all patients.
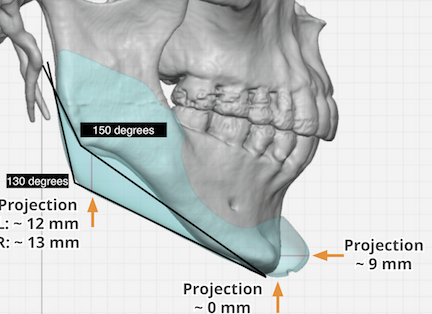
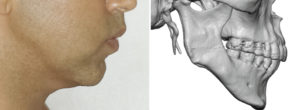 Case Study: This male presented for lower facial reshaping. He was bothered by his short chin and lower Jaw. He had indistinct jaw angle and a full neck with overall thick facial tissues. He desired and improved lower jaw and neck shape. His 3D CT scan showed high jaw angles and a short and slightly vertically long chin. Comparing his 3D CT scan with his side profile the correlation between his high jaw angles and his facial appearance could be clearly seen. His gonial angle measurement was over 150 degrees.
Case Study: This male presented for lower facial reshaping. He was bothered by his short chin and lower Jaw. He had indistinct jaw angle and a full neck with overall thick facial tissues. He desired and improved lower jaw and neck shape. His 3D CT scan showed high jaw angles and a short and slightly vertically long chin. Comparing his 3D CT scan with his side profile the correlation between his high jaw angles and his facial appearance could be clearly seen. His gonial angle measurement was over 150 degrees.
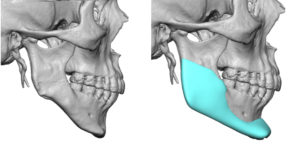
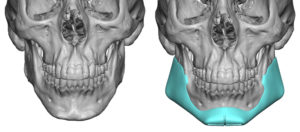
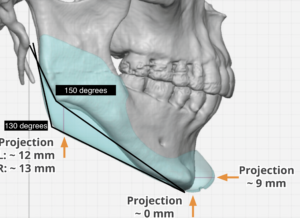 Using his 3-D CT scan a custom jawline implant was designed to bring his high jaw angles down, bring his chin forward and up as well as create a smooth linear connection between the two jaw points. At 12 to 13 mm of jaw angle lengthening per side his gonial angle measurements dropped from 150° to 130°.
Using his 3-D CT scan a custom jawline implant was designed to bring his high jaw angles down, bring his chin forward and up as well as create a smooth linear connection between the two jaw points. At 12 to 13 mm of jaw angle lengthening per side his gonial angle measurements dropped from 150° to 130°.
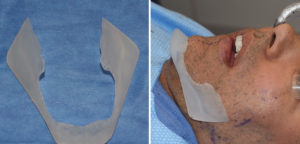
 Under general anesthesia a combination of a submental and bilateral intraoral incisions were used for implant placement. Because of the size of the jaw angle implant portion a geometric midline split technique was used with a front to back insertion technique. The implant was reunited in the midline through the submental incision and secured with two screws, one on each side of the split. He also underwent multiple facial defatting procedures of the cheeks and neck.
Under general anesthesia a combination of a submental and bilateral intraoral incisions were used for implant placement. Because of the size of the jaw angle implant portion a geometric midline split technique was used with a front to back insertion technique. The implant was reunited in the midline through the submental incision and secured with two screws, one on each side of the split. He also underwent multiple facial defatting procedures of the cheeks and neck.

 There is always a debate as to how much vertical lengthening should be done to the jaw angles. While gonial angle measurements have relevance how the masseter muscle will respond to the amount of vertical lengthening must always be considered. As excessive vertical jaw angle lengthening may be associated with failure of the masseter muscle to follow. (known as masseter muscle dehiscence or implant reveal) There is no, as of yet, exact known amount of vertical lengthening that is associated with increased or decreased probability of creating masseter muscle dehiscence. That will vary with each patient and their are anatomy. Suffice it to say large amounts of vertical jaw angle lengthening are more likely to do so than smaller amounts.
There is always a debate as to how much vertical lengthening should be done to the jaw angles. While gonial angle measurements have relevance how the masseter muscle will respond to the amount of vertical lengthening must always be considered. As excessive vertical jaw angle lengthening may be associated with failure of the masseter muscle to follow. (known as masseter muscle dehiscence or implant reveal) There is no, as of yet, exact known amount of vertical lengthening that is associated with increased or decreased probability of creating masseter muscle dehiscence. That will vary with each patient and their are anatomy. Suffice it to say large amounts of vertical jaw angle lengthening are more likely to do so than smaller amounts.
Highlights:
- Custom jawline implant designs in the high gonial angle patient require vertical jaw angle lengthening.
- The amount of vertical jaw angle lengthening vs the risk of masseteric muscle dehiscence must be carefully considered.
- The change in the gonial angle compared to the vertical angle lengthening is roughly 2 degree per every 1mm of vertical length. (2:1)
- Derotating the high mandibular angle patient must also consider whether the vertical length of the chin needs also to be shortened.
Dr. Barry Eppley
Indianapolis, Indiana