

Background: Plagiocephaly is a common and most recognized developmental skull shape deformity. It is typically seen as a flattening on one side of the back of the head that wraps around the side onto the posterior temporal region. This is why the ear on the affected side is always displaced a bit more forward. In some cases the opposite more normally developed side is concurrently protrusive…but this is uncommon and poses a more difficult aesthetic challenge if present.
When correcting the plagiocephalic back of the head the typical approach is to create an implant design that corrects the flat side based on the fullness of the other side. (mirror image) While this works well for many, some cases of plagiocephaly are associated with degrees of flatness on both sides. Such that even the more projected side is too flat. This can be appreciated in both right and left side views where both sides look too flat. Often with this flatness the crown height is high. (tall)
In augmenting a flat back of the head, including the good side, the pertinent design questions become how much augmentation is needed and what is the level of the maximum projection line.
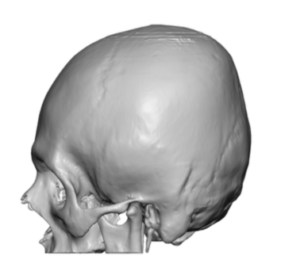
 Case Study: This male desired to correct a flat back of his head which had bothered him since he was a child. His 3D CT scan showed a flat and tall back of the head with a flatter left side. His biparietal width was expanded as would be expected with an overall flat back of the head.
Case Study: This male desired to correct a flat back of his head which had bothered him since he was a child. His 3D CT scan showed a flat and tall back of the head with a flatter left side. His biparietal width was expanded as would be expected with an overall flat back of the head.
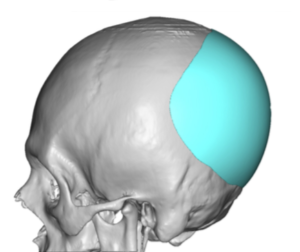
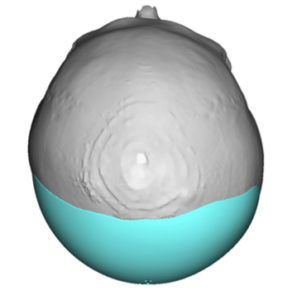
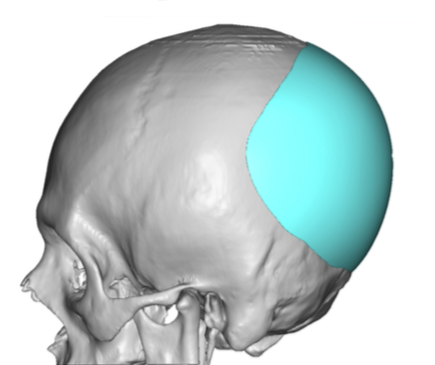
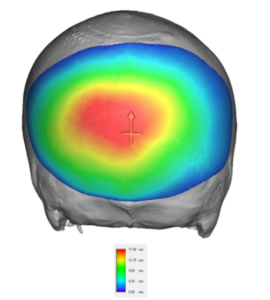 Using his 3D CT scan a custom skull implant was designed to build up the back of the head with a maximum projection on the flattest side of 17mms. This maximum point of projection was at the level of the flattest part of the back of the head which corresponded to the mid-forehead on the front of the skull. This resulted in an implant that was longer from side to side that it was from top to bottom. Total implant volume was 150ccs.
Using his 3D CT scan a custom skull implant was designed to build up the back of the head with a maximum projection on the flattest side of 17mms. This maximum point of projection was at the level of the flattest part of the back of the head which corresponded to the mid-forehead on the front of the skull. This resulted in an implant that was longer from side to side that it was from top to bottom. Total implant volume was 150ccs.

 Under general anesthesia and in the prone position a 9cm long beveled (paralleling the existing hair shafts) scalp incision was made just above the nuchal ridge line. Once down on the bone very wide subperiosteal underling of the scalp was done. This always needs to be larger than the footprint of the implant design. This was particularly relevant in this case as the implant must be initially inserted sideways with the longest part (side to side) going in first. Once inside it must be turned 90 degrees for the proper orientation.
Under general anesthesia and in the prone position a 9cm long beveled (paralleling the existing hair shafts) scalp incision was made just above the nuchal ridge line. Once down on the bone very wide subperiosteal underling of the scalp was done. This always needs to be larger than the footprint of the implant design. This was particularly relevant in this case as the implant must be initially inserted sideways with the longest part (side to side) going in first. Once inside it must be turned 90 degrees for the proper orientation.

 Bony asymmetry of the back of the head is most effectively improved by a custom skull implant. From a volumetric standpoint that has never proven to require more implant than the scalp can stretch to accommodate it in my experience. But when combined with an overall lack of adequate projection even on the good side, the volume of the implant must be increased to the point of maximal scalp stretch which for many patients is in the 150cc volume range.
Bony asymmetry of the back of the head is most effectively improved by a custom skull implant. From a volumetric standpoint that has never proven to require more implant than the scalp can stretch to accommodate it in my experience. But when combined with an overall lack of adequate projection even on the good side, the volume of the implant must be increased to the point of maximal scalp stretch which for many patients is in the 150cc volume range.
Case Highlights:
1) Plagiocephaly most commonly affects the back of the head and can be associated with an overall flatness as well.
2) A custom skull implant design can simultaneously correct back of head asymmetry as well as provide overall increased back of head projection.
3) The volumetric addition to the back of the head should generally not exceed 150cc unless a first stage scalp expansion has been done.
Dr. Barry Eppley
Indianapolis, Indiana