

Background: The shape of the head is typically rounder regardless of the view to which it is seen. In the profile view it has an oblong curved convex shape. When seen from behind the shape of the head is fairly round. When looked at front the front, which is how most people see their head, it can have a variety of shapes from round, more square in form or having a very slight midline peak.
One type of head shape deformity is that of the peaked or inverted V-shape skull which is seen in the front view. As the name implies there is a midline crest or high point surrounded by a sloped bone shape to the sides. The key question is whether this is due to the development of prominent bony sagittal crest (the sides are normal height but the midline is too high) or whether the the midline height is normal but the sides (bony temporal lines) are too low. (parasagittal deficiency) Or even possibly a combination of both. The best way to make that determination is computer imaging to assess how the head shape looks between sagittal crest reduction, parasagittal augmentation or combing both types of skull shape changes.
For some men and most women the true shape of the head is not visible due to hair. But for many men affected by a head shape concern the lack of hair or a short hairstyle leaves the head shape exposed. Men often compensate for head shape issues by growing out what hair they have or wearing some form of a head covering. (e.g., hat) I have heard many a man talk about all the different hats they have and having to always choose a hat that matches their outfit when they go out in public.
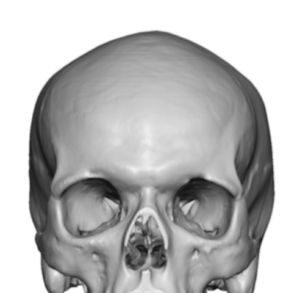
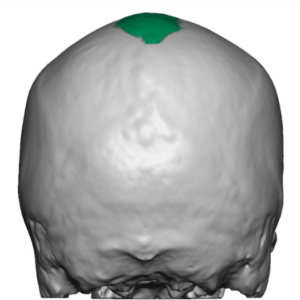
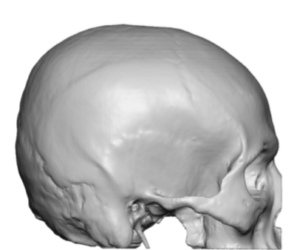 Case Study: This male was bothered by the shape of his head which has an inverted V-shape in the front and a downward slope in the side view in the back. His 3D CT scan showed the bone basis for his skull shape which was primarily a parasagittal deficiency with only a slight sagittal crest.
Case Study: This male was bothered by the shape of his head which has an inverted V-shape in the front and a downward slope in the side view in the back. His 3D CT scan showed the bone basis for his skull shape which was primarily a parasagittal deficiency with only a slight sagittal crest.
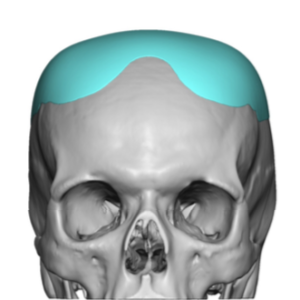
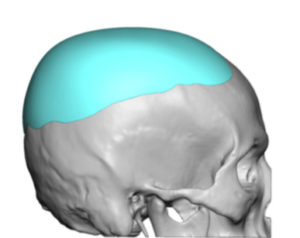 Using his 3D CT scan a custom skull implant was designed to fill in the parasagittal deficiency as well s wrap round the upper back of the head. The midline sagittal area was largely covered by it incorporated a 4mm sagittal crest reduction.
Using his 3D CT scan a custom skull implant was designed to fill in the parasagittal deficiency as well s wrap round the upper back of the head. The midline sagittal area was largely covered by it incorporated a 4mm sagittal crest reduction.
 Under general anesthesia and in the supine position a 9cm long horizontal scalp incisions was made at the back end of the sagittal crest. Through this incision a sagittal crest reduction was initially done.
Under general anesthesia and in the supine position a 9cm long horizontal scalp incisions was made at the back end of the sagittal crest. Through this incision a sagittal crest reduction was initially done.


 The placement of the custom skull implant was then done in a folded fashion through the same incision. It was unfolded once inside the pocket, centrally positioned and secured in that position with two microscrews. A drain was placed prior to scalp closure.
The placement of the custom skull implant was then done in a folded fashion through the same incision. It was unfolded once inside the pocket, centrally positioned and secured in that position with two microscrews. A drain was placed prior to scalp closure.

In the inverted V shape skull deformity a custom implant design that incorporates even a small amount of sagittal crest reduction creates an immediate pleasing diametrically changed head shape. The custom skull implant is responsible for about 90% of the change.
Case Highlights:
1) A peaked head shape deformity may be due to a midline sagittal crest, a bilateral parasagittal deficiency or a combination of both.
2) Many peaked or inverted V-shaped head from the frontal view is due to a major parasagittal deficiency and a minor sagittal crest elevation.
3) A custom parasagittal-parietal skull implant design combined with a sagittal crest reduction produces a better result than either one alone.
Dr. Barry Eppley
Indianapolis, Indiana