

Background: Asymmetry of any paired facial bony structure is not uncommon including the jaw angles. The jaw angles create the width of the lower face in the front view and the slope of the mandibular plane angle in the side view. Because of their bilateral protruding (or lack of protrusion) nature it is fairly easy to see when jaw angle asymmetry exists. While many people have some degree of bony jaw angle asymmetry, which I see all the time in 3D CT scans for any type of custom facial implant design, certain jaw surgery procedures can either create it or magnify its pre-existence.
The sagittal split ramus osteotomy (SSRO) of the mandibular ramus is the most common surgical procedure that can create jaw angle asymmetries. Splitting the bony jaw angle sagittally, moving the distal tooth bearing bone section (typically forward) and then putting the two jaw angle segments back together of both sides creates the ideal opportunity to unknowingly create shape differences between the two sides. Changes in the bony jaw angle shape cm also occur due to bone resorption with partial devascularization of the bone or from the placement of protruding hardware.
In attempting to correct jaw angle asymmetry after an SSRO has well healed (6 to 12 months later), a 3D CT scan should he done for an accurate evaluation. Panorex and cephalometric x-rays are 2D imaging studies that do not provide an adequate detailed assessment of the bony anatomy of the jaw angles. In addition trying to guess or eyeball how to fix it from an external assessment with standard jaw angle implants is a recipe for just creating a different asymmetry problem. As a general rule it is always good to remember one of the many basic rules in plastic surgery…’the smaller the problem is the more precise the surgery for it must usually be’.
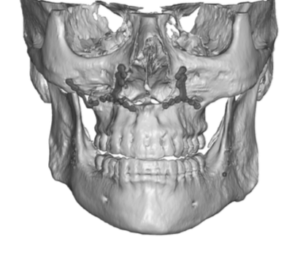
 Case Study: This male has double jaw surgery years ago and had always been bothered by his right jaw angle asymmetry since. A 3D CT scan showed the clear difference between the good side (patient left) and the bad side. (patient right)
Case Study: This male has double jaw surgery years ago and had always been bothered by his right jaw angle asymmetry since. A 3D CT scan showed the clear difference between the good side (patient left) and the bad side. (patient right)
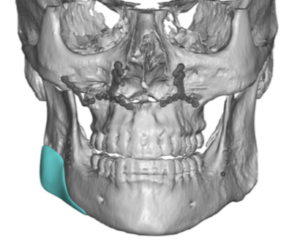
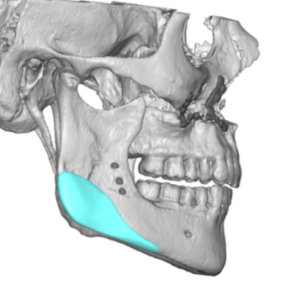
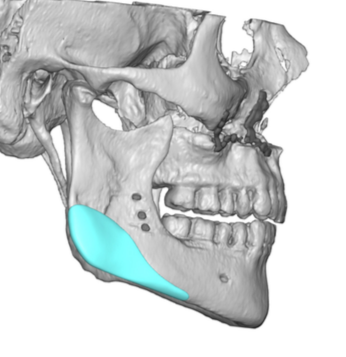
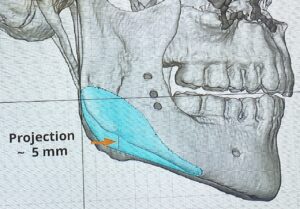 Using the 3D CT scan a right jaw angle implant was designed that initially matched the left side identically. But for fear that of an over correction the patient denied to have the implant slightly smaller than that of the left side in terms of width and how far the asymmetry came forward into the body of the mandible.
Using the 3D CT scan a right jaw angle implant was designed that initially matched the left side identically. But for fear that of an over correction the patient denied to have the implant slightly smaller than that of the left side in terms of width and how far the asymmetry came forward into the body of the mandible.

 Under general anesthesia and through a right posterior vestibular incision the right jaw angle implant was placed with some difficulty. Being so small getting it into the right place over the distance jaw angle region through the limited visualization of the incision was not easy. It may always look so on an implant design. But it is important to remember that the jaw angle implant is unique of all the bony facial implants…the working end of the implant is the furtherest away from the location of the incision. But eventually good implant positioning was achieved and double screw fixation doe through a percutaneous technique.
Under general anesthesia and through a right posterior vestibular incision the right jaw angle implant was placed with some difficulty. Being so small getting it into the right place over the distance jaw angle region through the limited visualization of the incision was not easy. It may always look so on an implant design. But it is important to remember that the jaw angle implant is unique of all the bony facial implants…the working end of the implant is the furtherest away from the location of the incision. But eventually good implant positioning was achieved and double screw fixation doe through a percutaneous technique.
It is hard enough with using a custom implant design and then getting the implant in the designed position to adequately correct jaw angle bony asymmetry. I would not think of doing so with any realistic hope using a standard implant with getting a comparative result.
Case Highlights:
1) Noticeable jaw angle asymmetry can occur after sagittal split mandibular osteotomies corrective surgery.
2) The nature of jaw angle asymmetries after surgical manipulation should be first evaluated with a 3D CT scan to appreciate the exact dimensions of the bony asymmetry.
3) A custom jaw angle implant design is the most precise method to try and obtain improved symmetry between the two sides with attention paid to the risk of overcorrection.
Dr. Barry Eppley
Indianapolis, Indiana