

Background: Chin augmentation is a general term that encompasses a variety of different techniques to do so. The two commonly used methods are an implant and an osteotomy. A wide variety of implant materials, styles and sizes are available to create almost every type of desired chin augmentation effect. For very significant chin augmentations beyond what an implant can do or for those that want to avoid having an implant the bony or sliding genioplasty is the other method. While there are advantages and disadvantages to each type of chin augmentation approach each method has its specific indications.
For some dimensional chin augmentation needs, it is possible and may be necessary to combine an implant with a bony genioplasty. This is usually done when the patient prefers a sliding genioplasty but does not want it to be too narrow or even wider than the original chin shape. It can also be done when it requires both to achieve the amount of horizontal augmentation desired, either during the primary procedure or as a secondary implant overlay.
Chin and lower lip tightness is always a potential postoperative concern with an intraoral approach that cuts through the mentalis muscle. It more commonly occurs in sliding genioplasty advancements where a bony step off is created and the mentalis muscle needs to be reapproxiomated. When it occurs surgeons attempt twi treat it with a variety of methods including steroid injections, hardware removal and scar releases. In the vast majority of cases, however, these methods don’t work as the actual diagnosis, a soft tissue deficiency, is not recognized. The concept of a,scar release will not work in the chin unless soft tissue volume is added into the dead space created by the release. This is best done by a fat graft.
Case Study: This young male had a significant chin augmentation history that initially began with a large (11mm) chin implant of which he was happy with the result. When he sought a rhinoplasty by another surgeon he convinced him that chin implants were ‘bad’ and he should have a sliding genioplasty replacement instead. During his rhinoplasty the chin implant was removed and an alleged 15mm sliding genioplasty was done. Due to an inadequate chin augmentation effect a 3D CT scan done later showed 6mm forward and 4mm downward chin bone movement. (hardly an adequate dimensional replacement for the original chin implant) In addition to a still inadequate horizontal chin projection it was now too long and he had significant chin tightness with lower lip restriction and volume loss. To help with his chin tightness the surgeon performed some form of a release and fat graft which provided no functional benefit.

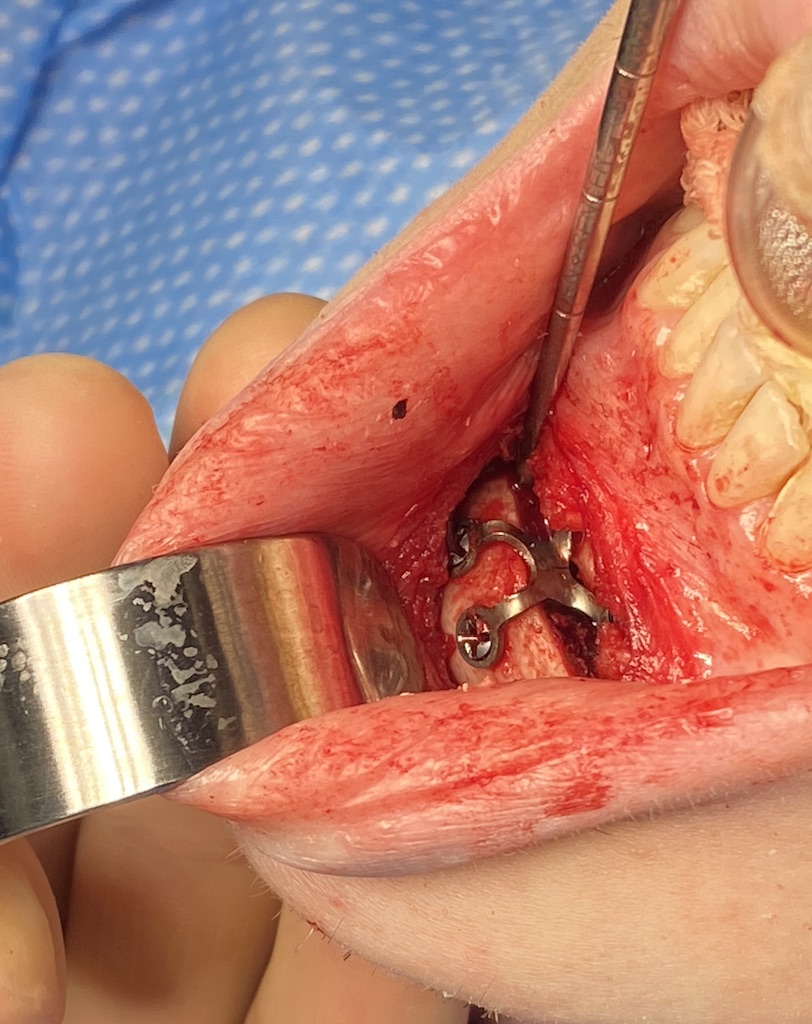
 Under general anesthesia the hardware from his first bony genioplasty was removed and the osteotomy line recut. The chin bone was then shortened (brought upward) 3mms and advanced 6mms and secured with a plate and 4 screws.
Under general anesthesia the hardware from his first bony genioplasty was removed and the osteotomy line recut. The chin bone was then shortened (brought upward) 3mms and advanced 6mms and secured with a plate and 4 screws.

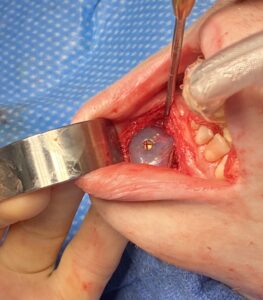 A 10mm mandibular glove chin implant , after being coated in Vancomycin antibiotic powder, was placed in front of the chin and secured with a midline screw.
A 10mm mandibular glove chin implant , after being coated in Vancomycin antibiotic powder, was placed in front of the chin and secured with a midline screw.


 Lastly to treat his chin and lower lip tightness a dermal-fat graft was harvested from the left flank and used an interpositional graft between the implant and the musculomucosal closure to treat the chin tightness.. A small piece of the dermal-fat graft was placed in the central lower lip for volume restoration.
Lastly to treat his chin and lower lip tightness a dermal-fat graft was harvested from the left flank and used an interpositional graft between the implant and the musculomucosal closure to treat the chin tightness.. A small piece of the dermal-fat graft was placed in the central lower lip for volume restoration.

 This combined autologous (sliding genioplasty and dermal-fat graft) and all-plastic (chin implant) approach took a maximal approach to treating every chin problem he had from his prior chin surgeries. (too vertically long, persistent horizontal deficiency and chin and lower lip tightness) It is interesting thats much could be done in the otherwise limited space of the small chin. The prior chin surgeries helped in that regard by inducing some soft tissue expansion.
This combined autologous (sliding genioplasty and dermal-fat graft) and all-plastic (chin implant) approach took a maximal approach to treating every chin problem he had from his prior chin surgeries. (too vertically long, persistent horizontal deficiency and chin and lower lip tightness) It is interesting thats much could be done in the otherwise limited space of the small chin. The prior chin surgeries helped in that regard by inducing some soft tissue expansion.
Case Highlights:
1) Bony genioplasties and chin implants can be used in combination to meet specific dimensional chin augmentation needs.
2) The use of dermal-fat grafts, while traditionally used to treat chin and lower lip tightness as a stand alone procedure, can be used as an interpositional graft between an implant and the intraoral closure foe the same purposes..
3) A triple genioplasty augmentation approach refers to aesthetic treatments of the bone, implant placement and soft tissue volume addition.
Dr. Barry Eppley
World-Renowned Plastic Surgeon