

Background: Cleft lip and plate deformities are one of the most common congenital facial deformities. It has a wide range of expressions but the near complete or complete cleft lip component is one consistent finding. The majority of cleft lip repairs are done in infancy within six months of birth in most countries.

 A variety of cleft lip repairs have been described over the years but the most common technique is the rotation-advancement procedure. The rotation refers to the downward rotation of the medial cleft lip element which is achieved by a back cut. The advancement refers to the inward movement of the lateral lip element behind and along the downwardly rotated medial lip. This places the scar line along the natural philtral column and up under the columella at the base of the nose.
A variety of cleft lip repairs have been described over the years but the most common technique is the rotation-advancement procedure. The rotation refers to the downward rotation of the medial cleft lip element which is achieved by a back cut. The advancement refers to the inward movement of the lateral lip element behind and along the downwardly rotated medial lip. This places the scar line along the natural philtral column and up under the columella at the base of the nose.
Despite the common use of the rotation-advancement type cleft lip repair, achieving adequate phitral length does not always occur. This can leave the left side of the lip vertically short with a v-shaped notch of the vermilion and excessive tooth exposure during smiling. Revising the inadequately rotated cleft lip is facilitated by the initial rotation-advancement repair.
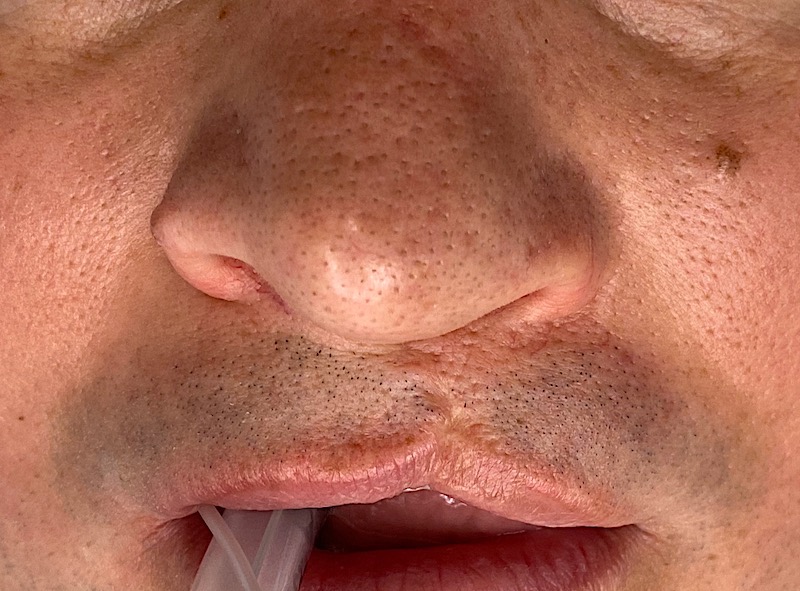
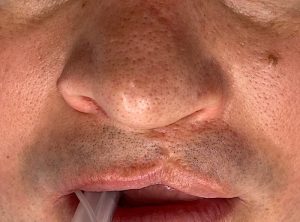 Case Study: This male was born with a left cleft lip and palate deformity which was repaired as an infant. He had no other repairs until he was seen at almost forty years old. He had a residual vertical philtral deficiency with an inverted v-shaped vermilion notch.
Case Study: This male was born with a left cleft lip and palate deformity which was repaired as an infant. He had no other repairs until he was seen at almost forty years old. He had a residual vertical philtral deficiency with an inverted v-shaped vermilion notch.

 Under general anesthesia the medial and lateral lip elements were separated along the philtral scar line in a full thickness manner. The medial lip element was further backcut across the base of the columella so that it could be rotated down further. The lateral lip element was the advanced in behind the opening created by the downward movement of medial lip element. Both sides of the lip were fully reassembled from the inner mucosa, muscle middle layer and the outer skin layer.
Under general anesthesia the medial and lateral lip elements were separated along the philtral scar line in a full thickness manner. The medial lip element was further backcut across the base of the columella so that it could be rotated down further. The lateral lip element was the advanced in behind the opening created by the downward movement of medial lip element. Both sides of the lip were fully reassembled from the inner mucosa, muscle middle layer and the outer skin layer.
 Once the height of the cupid’s bow was made as even as possible with the non cleft lip side, vermilion adjustments were done. The larger lateral lip vermilion was reduced by an internal horizontal mucosal excision while a fat graft was placed into the medial lip vermilion to add fullness.
Once the height of the cupid’s bow was made as even as possible with the non cleft lip side, vermilion adjustments were done. The larger lateral lip vermilion was reduced by an internal horizontal mucosal excision while a fat graft was placed into the medial lip vermilion to add fullness.
His results demonstrate that in many cleft lip revisions an effective improvement does not come by a few limited maneuvers. Like a primary
Case Highlights:
1) Cleft lip revisions in an adult when both lip elements are under rotated requires a procedure similar to the primary cleft lip repair.
2) The rotation-advancement cleft lip repair technique is the most assured method of establishing symmetric philtral length even in revisional surgery.
3) Even with successful philtral lengthening adjustments of the vermilion fullness on each side of the lip repair will still be needed.
Dr. Barry Eppley
Indianapolis, Indiana