


Background: The metopic suture runs down the midline on the frontal bone of the forehead. At its back end is the bregma where it intersects with the transverse coronal sutures. At its front end it intersects with the nasal bones. Its function in the neonate is to facilitate passage through the birth canal by allowing malleability of the head. Once this function has been achieved the metopic suture fuses and disappears within the first year of life. But if the skull bones grow too rapidly in utero the metopic suture may fuse before birth restricting its width development. This creates the well known metopic craniosynostosis or trigonocephaly head shape.
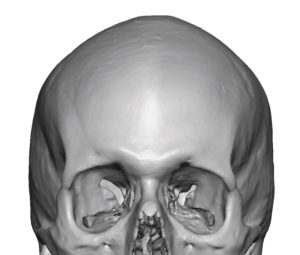
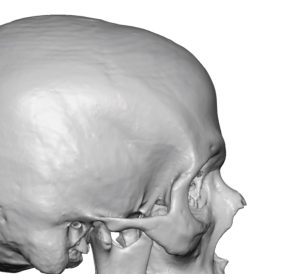 But there is a spectrum of premature sutural fusions which have lesser degrees of head shape deformations as the suture fusion is partial or incomplete. These typically present as ridges or crests of which sagittal crests are the most commonly seen. But such ridges from incomplete sutural fusion can also occur in the forehead from the metopic suture. This palpable ridge starts behind the hairline and extends into the upper half of the forehead. It can be very slight to a more pronounced ridge. A visible suture line will not be seen unless it is reduced in which the suture line becomes apparent, demonstrating that an incomplete premature sutural fusion existed. 3D CT scans will show the ridge without a visible suture line.
But there is a spectrum of premature sutural fusions which have lesser degrees of head shape deformations as the suture fusion is partial or incomplete. These typically present as ridges or crests of which sagittal crests are the most commonly seen. But such ridges from incomplete sutural fusion can also occur in the forehead from the metopic suture. This palpable ridge starts behind the hairline and extends into the upper half of the forehead. It can be very slight to a more pronounced ridge. A visible suture line will not be seen unless it is reduced in which the suture line becomes apparent, demonstrating that an incomplete premature sutural fusion existed. 3D CT scans will show the ridge without a visible suture line.

 Case Study: This adult male had a palpable bony ridge from the top of his head down to the middle of the forehead. It was a ridge of 3 to 4mms in height. Given its length and that it went around a curve I(upper forehead-skull transition) a scalp incision was marked halfway along its length just behind the hairline.
Case Study: This adult male had a palpable bony ridge from the top of his head down to the middle of the forehead. It was a ridge of 3 to 4mms in height. Given its length and that it went around a curve I(upper forehead-skull transition) a scalp incision was marked halfway along its length just behind the hairline.

 Under general anesthesia and through the small zigzag scalp incision, the forehead ridge was reduced with a guarded high speed burr. Then turning around 180 degrees the anterior sagittal ridge was similarly reduced.
Under general anesthesia and through the small zigzag scalp incision, the forehead ridge was reduced with a guarded high speed burr. Then turning around 180 degrees the anterior sagittal ridge was similarly reduced.
 Once the ridge was reduced the metopic suture line could be seen, demonstrating that this was a very limited fusion of the suture. A two layer scalp closure was then done with a circumferential head wrap.No drain was used.
Once the ridge was reduced the metopic suture line could be seen, demonstrating that this was a very limited fusion of the suture. A two layer scalp closure was then done with a circumferential head wrap.No drain was used.
Compared to a sagittal crest the metopic ridge is far more rarely seen. This would be consistent with the differences in the occurrence between congenital sagittal and metopic craniosynostoses so similar findings would also occur with more minor ridge developments as well.
Case Highlights:
1) Microform metopic craniosynostosis can present as a limited midline ridge anterior to the coronal sutures extending down into the forehead.
2) A small frontal scalp incision midway between the length of the raised bony ridge provides dual access for complete skull and forehead ridge reduction.
3) Burring reduction of a midline metopic skull ridge can safely remove up to 5mms in most cases.
Dr. Barry Eppley
World-Renowned Plastic Surgeon