

Background: Custom jawline implants can be made of a variety of materials each with their own advantages and disadvantages. One of these materials is porous polyethylene or Medpor. It offers a firm soft tissue adhesion to its surface to which that advantage over other materials which do not develop this strong adhesion is not clinically clear. Be that as it may it does occur albeit more strongly on the outer surface of implant exposed to the overlying soft tissues. On the underside of the Medpor implant bone ingrowth does not occur but a thick capsule does develop.
Understanding these tissue reactions to Medpor material becomes more than of biologic interest if the need arises to either adjust the position of the implant or remove/replace it. Like any other facial implant this potential need is not rare and occurs equally amongst all implant materials. When this need arises it is an implant design (shape and size) issue and not one of its material composition.
This becomes most relevant the larger the implant is and a custom jawline implant represents one of the largest facial implants possible. Designing a new custom jawline implant to replace it is relatively easy since the indwelling implant provides the guidance to determine how to make a new jawline implant design better. Getting the Medpor jawline implant out poses the challenge but understanding its enveloping tissue reaction to its surface provides the technical manuevers in doing so.
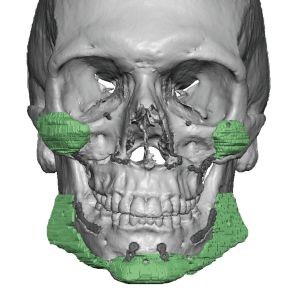
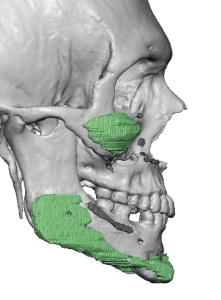 Case Study: This male patient had a jaw history of orthognathic surgery (sagittal split and LeFort I osteotomies) and placement of a custom Medpor jawline implant. He felt it was too big and the original implanting surgeon attempter to do a jawline reduction in situ. He developed an infection of the right jaw angle which was subsequently removed. (This 3D CT scan was taken before the revision and the loss of the right jaw angle part of the implant)
Case Study: This male patient had a jaw history of orthognathic surgery (sagittal split and LeFort I osteotomies) and placement of a custom Medpor jawline implant. He felt it was too big and the original implanting surgeon attempter to do a jawline reduction in situ. He developed an infection of the right jaw angle which was subsequently removed. (This 3D CT scan was taken before the revision and the loss of the right jaw angle part of the implant)
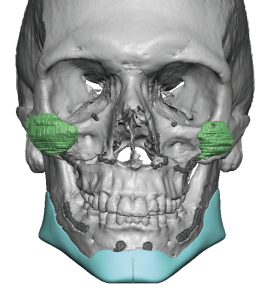
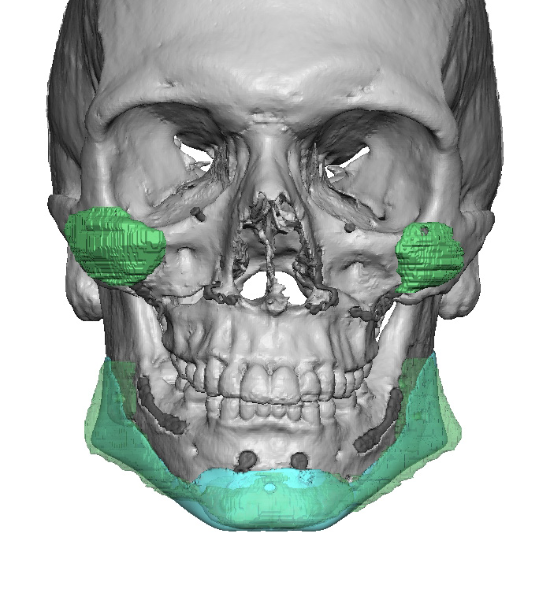
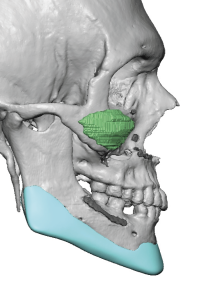 To replace the indwelling Medpor implant with a smaller size a new custom jawline implant was designed out of solid silicone as its replacement. The new implant was designed to be smaller in size with less jaw width.
To replace the indwelling Medpor implant with a smaller size a new custom jawline implant was designed out of solid silicone as its replacement. The new implant was designed to be smaller in size with less jaw width.
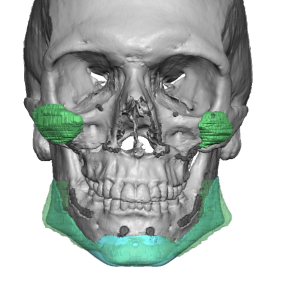
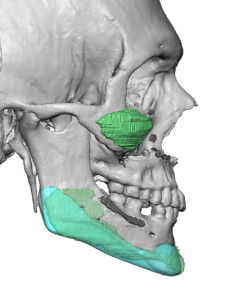 The best way to determine the change is to overlay the new implant design over the existing indwelling implant.
The best way to determine the change is to overlay the new implant design over the existing indwelling implant.

 Under general anesthesia the existing submental skin and inntraoral incisions were opened and the implant exposed. (on the right jaw angle side there was no implant) To begin the implant removal the chin section was initially split with a scalpel and the implant lifted off from the underlying bone back as far along the jawline as possible on both sides. In so doing any screws can be found and either can be unscrewed before the implant is lifted off or the implant can be pushed through the screws and the more exposed screw lengths can be rotated out of the bone with a needle holder. This is the safest way to begin to remove Medpor in the plane between the implant and the bone. This mobilizes the implant and provides a handle to do the more tedious separation of the overlying soft tissues from the external surface of the implant. In the chin area one has to be careful about the adherence of the implant to the mental nerve superiorly and the close association of the passage of the marginal nerve brain of the facial nerve in the lateral chin tissues. Back at the jaw angles the real danger is along the inferior border in front of the masseter muscle where the facial artery crosses over into the face. Unseen the facial artery can be firmly attached to the implant by the soft tissue adhesions, risking laceration of the artery when trying to remove the implant. While not a life threatening intraoperative problem, such bleeding can be difficult to control in the limited visibility of the intraoral access.
Under general anesthesia the existing submental skin and inntraoral incisions were opened and the implant exposed. (on the right jaw angle side there was no implant) To begin the implant removal the chin section was initially split with a scalpel and the implant lifted off from the underlying bone back as far along the jawline as possible on both sides. In so doing any screws can be found and either can be unscrewed before the implant is lifted off or the implant can be pushed through the screws and the more exposed screw lengths can be rotated out of the bone with a needle holder. This is the safest way to begin to remove Medpor in the plane between the implant and the bone. This mobilizes the implant and provides a handle to do the more tedious separation of the overlying soft tissues from the external surface of the implant. In the chin area one has to be careful about the adherence of the implant to the mental nerve superiorly and the close association of the passage of the marginal nerve brain of the facial nerve in the lateral chin tissues. Back at the jaw angles the real danger is along the inferior border in front of the masseter muscle where the facial artery crosses over into the face. Unseen the facial artery can be firmly attached to the implant by the soft tissue adhesions, risking laceration of the artery when trying to remove the implant. While not a life threatening intraoperative problem, such bleeding can be difficult to control in the limited visibility of the intraoral access.
The entire remaining Medpor implant was able to be removed and the new custom jawline implant placed.
As a facial implant material the limitations of Medpor are its rigidity and soft tissue adherence. Both of these material characteristics may have certain advantages but when it is needed to be removed they are disadvantages. It is one thing to remove an isolated chin or jaw angle Medpor implant but another when it is an entire wrap around jaw implant. While it can be successfully removed it takes experience to avoid inadvertent neurovascular structure damage. Part of that is knowing what can happen which is the best way too avoid it.
Case Highlights:
1) A prior custom jawline implant design goes a long way in determining how to make an improved jawline implant replacement design.
2) Medpor jawline implants can be technically challenging to remove but there are various maneuvers that can make it a successful explantation.
3) The tissue pocket created by a Medpor jawline implant removal is usually more than adequate for the new jawline implant placement.
Dr. Barry Eppley
Indianapolis, Indiana